Background
Corticosteroids are used to treat inflammatory manifestations of many rheumatologic conditions. Doses necessary to control disease are frequently high (e.g., 1 mg/kg or greater), and therapy may be maintained for prolonged periods of weeks to months. In this setting, one out of every two to three patients prescribed steroids may develop psychiatric symptoms including psychosis, mania, delirium, and depression. The most common symptoms reported with corticosteroid therapy are hypomania, mania, and psychosis.1
Psychiatric Symptoms Associated with Corticosteroids
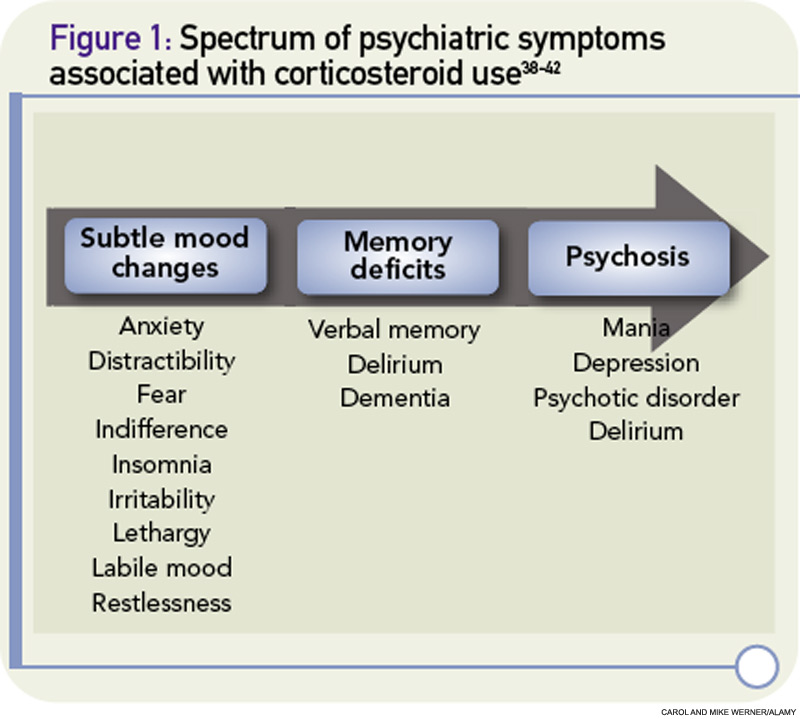
Psychiatric symptoms have been documented in association with the use of corticosteroids since these agents were first introduced in the 1950s.2 Corticosteroid-induced psychosis refers to a spectrum of psychiatric symptoms ranging from subtle mood changes to memory deficits to frank psychosis that can occur at any time during treatment (See Figure 1, p. 40).3 Mania and hypomania are reported most commonly (35%), followed by depressive symptoms (28%) and psychotic reactions (24%).2 Psychiatric symptoms typically develop three to four days after the initiation of corticosteroid therapy, although symptoms can occur at any time, including after cessation of therapy.
Symptoms may last a few days or persist for three weeks or more.2 A prospective study of outpatients with pulmonary disease who received 40 mg or more of corticosteroids for at least a week demonstrated a significant increase in measurable manic symptoms. The study also identified a subset of patients who developed dysphoric symptoms. These patients met criteria for post-traumatic stress disorder and were more likely to discontinue corticosteroids due to difficulties tolerating the mood symptoms.4
The pathophysiology of corticosteroid-induced psychosis remains poorly understood, although it is generally accepted that abnormalities of the hypothalamo–pituitary–adrenal (HPA) axis can result in mood disorders. For example, syndromes involving excess or inadequate cortisol production can have psychiatric manifestations. Cushing’s syndrome is associated with anxiety, euphoria, depression, and psychosis, whereas Addison’s disease can produce fatigue, low energy, decreased appetite, and symptoms consistent with neurovegetative symptoms of depression.
In the 1970s and 1980s, the psychiatric community showed interest in the use of the dexamethasone suppression test for the diagnosis of endogenous versus characterologic depression. Although the test has not been incorporated into standard care, it nevertheless points to an important relationship between the regulation of glucocorticoid production and mood disturbance.5 Whether corticosteroid-associated psychiatric symptoms are related to hippocampal effects, suppression of the HPA by dopamine neurotransmission, or other direct or indirect effects of corticosteroids is not well understood.6-8