He explained how, with ballooning wait times across rheumatology practices nationally, an increasing need exists to be more selective about the patients accepted to be seen in clinic. Data for rheumatology clinics at Duke University shows median wait times have increased to 160 days as of 2023 (Figure 1, below).
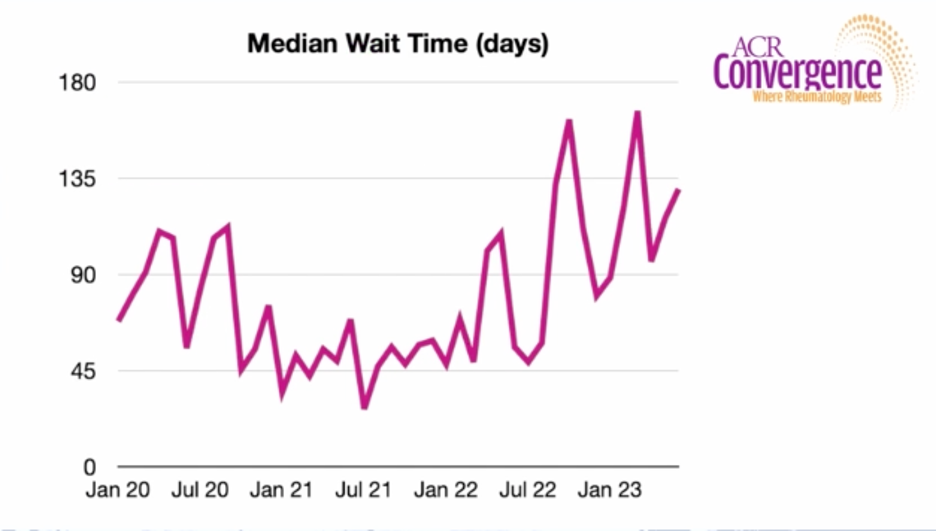
Figure 1: The median wait time at Duke University rheumatology clinics
Additionally, the longer the wait time, the higher percentage of patients who will no show or not attend the visit. The no-show rate is around 15% for patients scheduled within 90 days, but doubles to 30% for patients waiting nine to 12 months for an appointment.



