“This one.” She held up the pinky finger on the other hand. “The edge is separating from the rest of the nail. I showed it to Dr. F. last year, and he said the fingernails are a window to our health. Since then I’ve been taking supplements.” She reached over to her pocketbook and pulled out a sheet of paper cataloguing more than a dozen herbs and vitamins. “Dr. F. said that I’d know when the Lyme infection was on the run when the nails began to heal.”
“And are the nails looking any better?” I asked.
“I sometimes think they are,” she replied.
The heart, lungs, throat, ears were normal. The thyroid gland was in its usual position, shaped like a miniature bow-tie just above the breast bone. There were no enlarged lymph nodes in the neck or under the armpits. The shoulders and elbows were … hmm … the skin over the back of the elbows was raised and slightly reddened. A thick silvery scale adhered to the coin-sized lesion. Psoriasis.
“I have a cream for that,” Ms. Corinth said as she pulled the gown down. “It works if I keep applying it every day, but I’ve run out.”
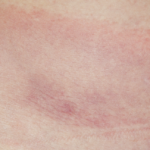
I asked her to lie down and, while palpating the left knee, confirmed that the red patch of skin in the mid-thigh I’d glimpsed earlier in our visit was also psoriasis. Interestingly, the discoloration and separation of the fingernail (i.e., onycholysis) and the small pits are also commonly associated with psoriasis.
I methodically assessed the motion in the knee. One measure of chronicity of fluid within a knee is the development of a joint contracture, the inability of a joint to fully flex or extend. Ms. Corinth’s knee lacked the last 10 degrees of normal extension and flexed to only 85 degrees. Patients who cannot normally flex or extend the knee fully often experience instability and frequent falls. Even with successful treatment, it will take months of physical therapy to restore function, that is, if the knee isn’t already cooked. Fluid within a knee this chronically inflamed can accelerate damage, destroying normal cartilage in less than a year.
“Dr. F. MRI’d the knee three months ago,” she said, reaching down and massaging the soft tissues. “He worried there might be something else inside keeping me from a full recovery, maybe a torn cartilage, but it was normal. Normal except for the Lyme fluid,” she added.