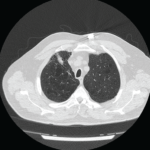
The patient was referred to a pulmonary specialist, who performed diaphragmatic ultrasound. The ultrasound revealed both reduction in diaphragm dome excursion and in diaphragm thickening fraction, consistent with bilateral diaphragm dysfunction, confirming diaphragmatic dysfunction and a diagnosis of shrinking lung syndrome (see Figure 1). Follow-up high-resolution CT showed no evidence of interstitial lung disease. Mycophenolate mofetil was initiated, in addition to prednisone.
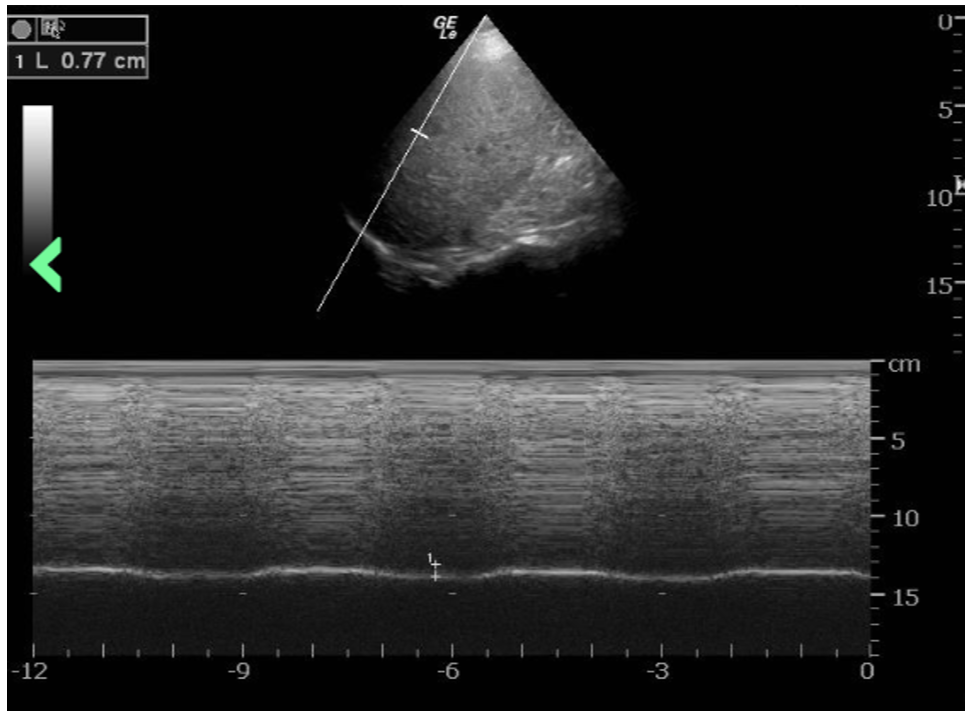
Figure 1: The ultrasound revealed a reduction in diaphragm dome excursion of 0.77 cm (normal value for deep inspiration: 4.8 cm) and in diaphragm thickening fraction, consistent with bilateral diaphragm dysfunction. (Click to enlarge.)
Repeat PFTs three months later demonstrated improvement, with FVC post 39%, FEV1 post 37%, FEV1/FVC post 92% predicted, TLC 50%, DLCO 38%, reduction in mean inspiratory pressure and decline of vital capacity from a seated to supine position.