Case Presentation
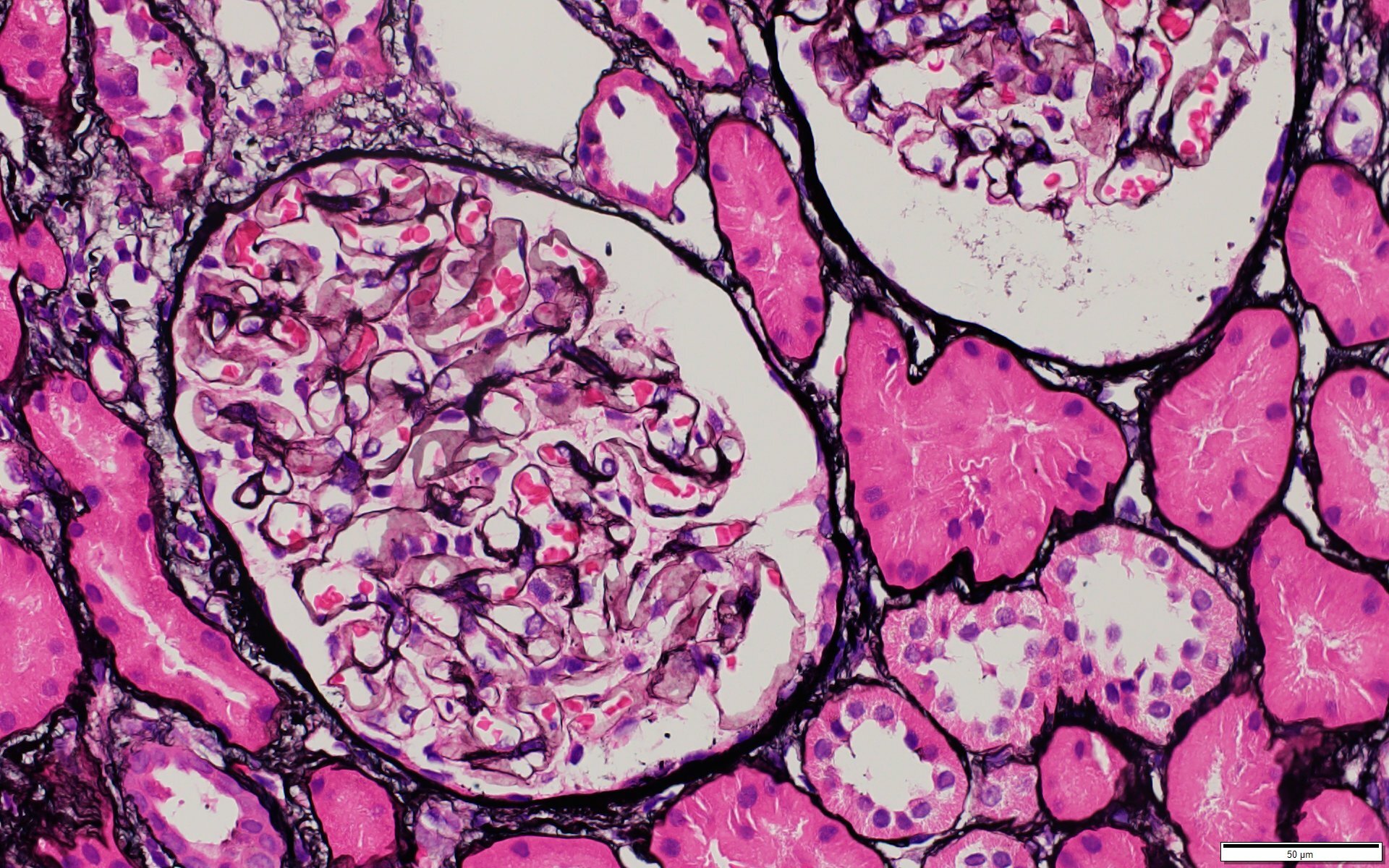
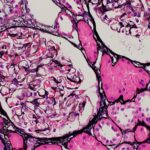
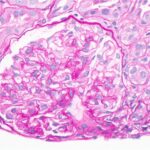
Figure 1: Jones Methenamine Silver (40x). Segmental spikes and holes noted in glomerular capillary loops. (Click to enlarge.)
A 34-year-old Angolese man presented with lower extremity edema, headache, malaise, arthralgias, rash, diarrhea and chest pain of six weeks’ duration. He previously was evaluated at an urgent care clinic and was prescribed an oral non-steroidal anti-inflammatory drug for chest pain and myalgias, with symptomatic improvement. Renal biopsy was concerning for classes II and V lupus nephritis, for which a rheumatologist was consulted.
His creatinine was 1.4 mg/dL (reference range [RR] 0.75–1.20 mg/dL for men) on admission. Liver function tests were normal, except for an isolated elevation in alkaline phosphatase confirmed to be of hepatic etiology, with a corresponding elevation in gammaglutamyl transferase.
The patient had recently been diagnosed with syphilis and treated with intramuscular penicillin a few weeks prior to his admission. His medical history included a prior diagnosis of COVID-19 and a remote history of malaria. Neither he nor his family had any history of autoimmune disease. He had not been taking any regular medications prior to admission. He denied use of illicit substances and had no travel outside the U.S. in several years. He reported being sexually active with male partners.
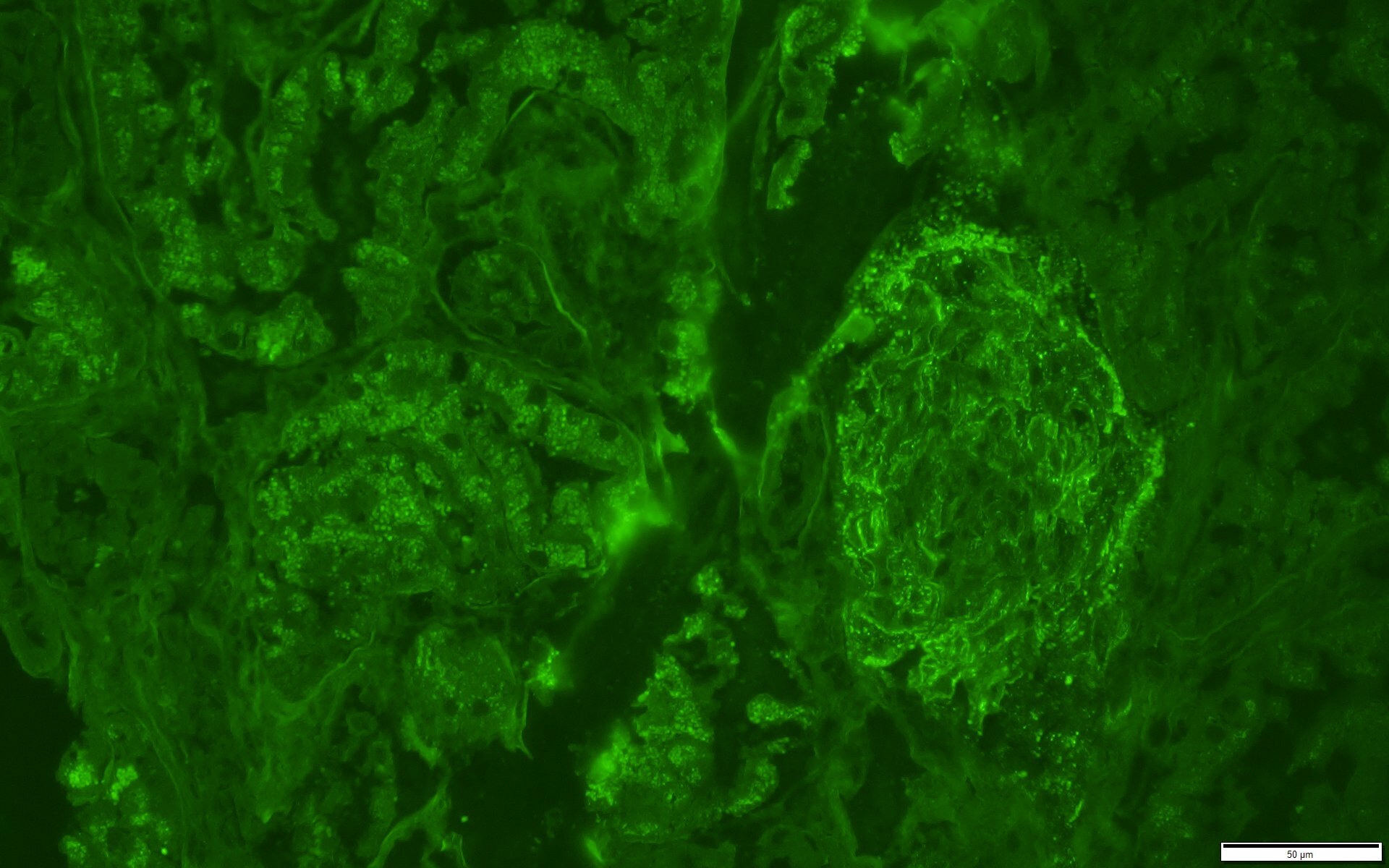
Figure 2: Immunofluorescence IgG Stain. IgG stain is positive in a granular pattern along capillary loop and rare mesangial areas. (Click to enlarge.)
On admission to our hospital, his exam revealed prominent bilateral axillary and bilateral inguinal lymph nodes, soft tissue swelling in both ankles and pretibial pitting edema. Examination found no appreciable rashes on the skin, including a normal genital exam with no ulcerative lesions. The patient denied malar rash, photosensitivity, Raynaud’s phenomenon, history of venous thromboembolic events, dry mouth, dry eye, history of seizure or stroke, history of cytopenias, nasal or oral ulcers, or hair loss.