Some of these patients have previously received a rheumatic diagnosis, such as anti-neutrophil cytoplasmic antibody (ANCA) vasculitis or relapsing polychondritis. However, these patients usually have very atypical presentations, and they are often glucocorticoid-dependent and poorly responsive to standard treatments.
Management of VEXAS
A key thrust of the guidance document is the need for collaboration in both diagnosing and managing such patients. “It’s really a team-based approach, with rheumatologists and hematologists as two of the most important coordinators,” says Dr. Koster. “It’s critical to have both perspectives because rheumatologists are not as comfortable with cytopenias, and hematologists are not as comfortable with managing and monitoring inflammatory states.”
Click to enlarge.
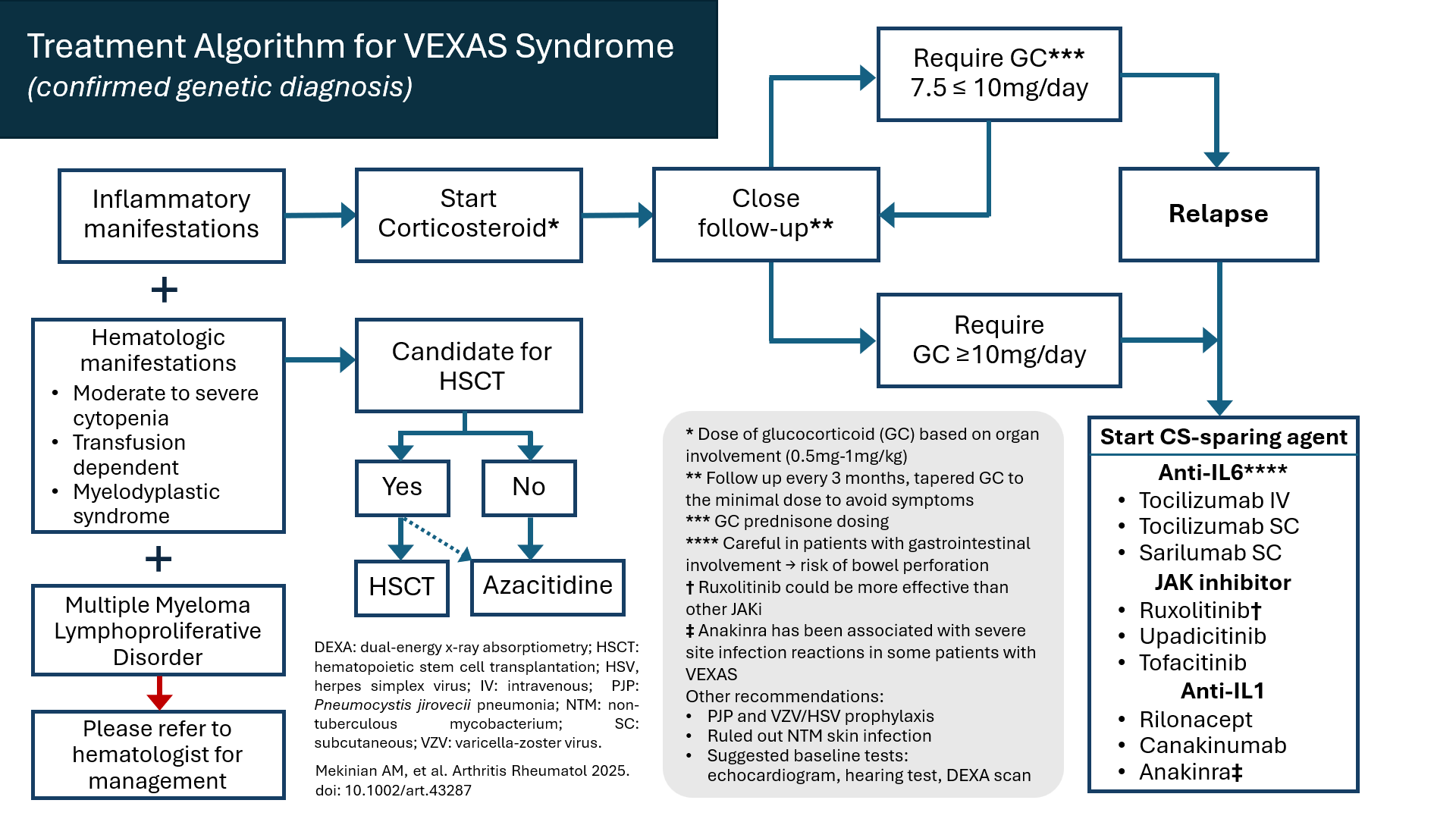
Disease activity in VEXAS can be defined by inflammation or worsening bone marrow failure. Treatment (see Figure 1) must encompass controlling inflammation, treating bone marrow failure and addressing any secondary complications from treatment (e.g., glucocorticoid toxicities).
Clinicians should start glucocorticoids for all patients with confirmed VEXAS and inflammatory manifestations. Glucocorticoid-sparing agents can be added as well, with some small studies and experience at expert centers showing potential benefits for anti-interleukin (IL) 6 or anti-IL-1 therapies, or Janus kinase (JAK) inhibitors. These agents, targeting inflammatory pathways, appear to be more effective than conventional disease-modifying anti-rheumatic drugs or B cell-directed therapies. Although many centers are using anti-IL-6 agents as the first-line therapy, not enough evidence exists to establish that definitively.



