click for large version
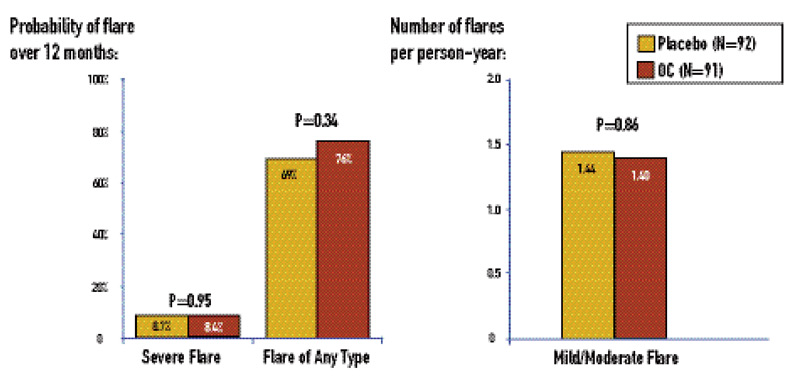
figure 1: Treatment for one year with OCs is unlikely to cause lupus flares (in inactive or stable-active patients without antiphospholid/anticardiolipin antibodies and/or history of thrombosis).1 Subjects were randomized to receive triphasic ethinylestradiol 35 mg plus norethindrone 0.5-1 mg for twelve cycles of 28 days.
Serious adverse events were rare in the cohort as a whole. There was one serious adverse event—a deep venous thrombosis—among the OC subjects, and three serious adverse events in the placebo group: one ocular thrombosis (after randomization but prior to taking placebo), one superficial thrombophlebitis, and one death a year after study drug (placebo) was discontinued due to severe flare at three months. None of the three subjects who experienced thrombotic adverse events had developed anticardiolipin antibodies.


