Presenting data from a scoping review of 63 studies in rheumatology, Dr. Barton emphasized that the data show shared decision making improves outcomes in rheumatic diseases by improving patient satisfaction with their treatment decisions, improving self-efficacy in the healthcare setting, improving patient-client trust and improving adherence to chosen treatment plans.1
However, she also pointed out that rheumatologists often do not engage in shared decision making. For example, in a study she conducted, 30% of adults with RA report poor communication around decision making with their clinicians, and factors independently associated with poorer communication include older patients, those with limited English proficiency, people with limited health literacy and those with a lower trust in their physician.2
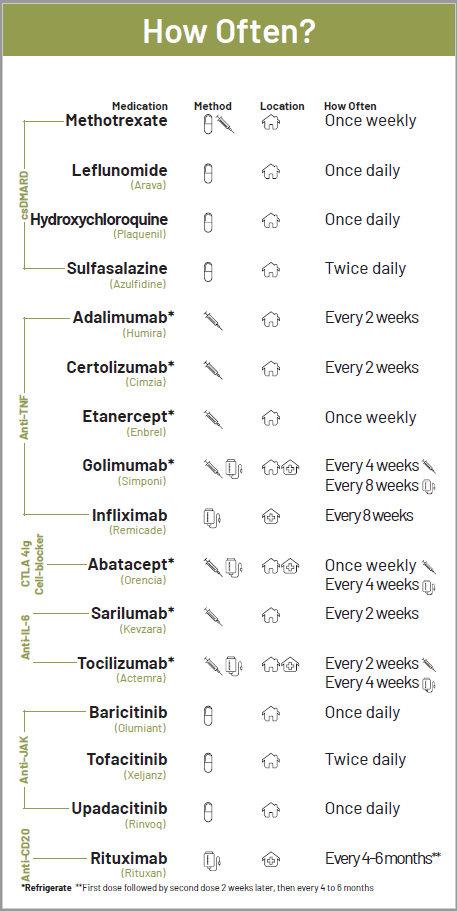
Research shows low literacy tools like this RA card increase knowledge, decrease decision conflict, and improve disease activity. (Click to enlarge.)



