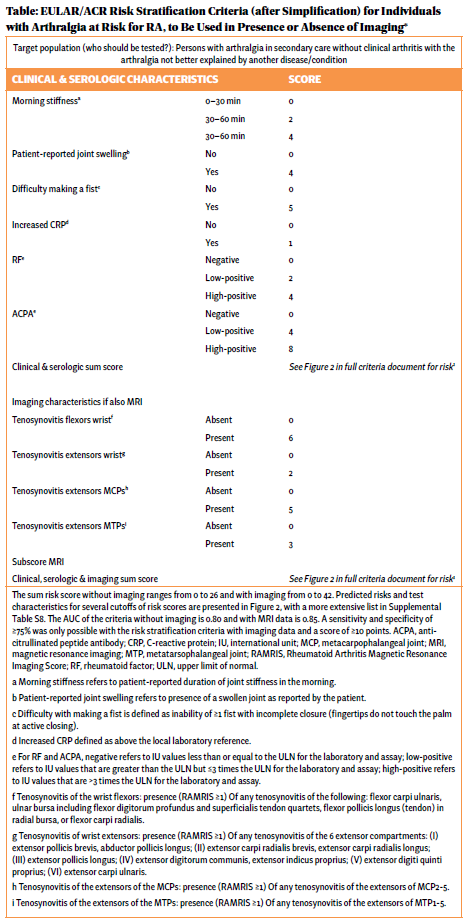
- Difficulty making a fist;
- Patient-reported morning stiffness;
- Patient-reported joint swelling;
- Increased C-reactive protein;
- Positive rheumatoid factor; and
- ACPA positivity.
Based on their respective predictive power, these were given different weights (e.g., four points for patient-reported joint swelling, five for difficulty making a fist, four points for low but positive ACPA, eight points for high-positive ACPA (see Table).
Click to enlarge.
The team also analyzed 10 ultrasound and 12 magnetic resonance imaging (MRI) variables, to see if imaging could improve discriminatory ability. Their specific analysis did not find that ultrasound further enhanced detection, but adding MRI improved the ability to accurately predict inflammatory arthritis.
Thus, a patient’s risk stratification criteria can be assessed just using clinical and serological parameters (with risk scores ranging from 0 to 26). Alternatively, adding additional MRI criteria, where available, can further improve accuracy (risk scores ranging from 0 to 42).

