Hydrocodone Combination Products
Rescheduling to control misuse & abuse
Hydrocodone combination products (HCPs) are among the most commonly prescribed opioid analgesics in the U.S., with 137 million prescriptions dispensed in 2013.5 Widespread use of hydrocodone has contributed significantly to opioid misuse and abuse. Since the Controlled Substances Act was passed in 1970, hydrocodone-only products have been Schedule II (C-II) controlled substances; whereas, HCPs have been Schedule III (C-III) controlled substances. Effective Oct. 6, 2014, a final rule by the U.S. Drug Enforcement Administration (DEA) moved HCPs from C-III to C-II, placing more restrictions on their use.6
Key changes to the rescheduling of HCPs:
- Prescriptions for HCPs that were issued on or after Oct. 6, 2014, must comply with requirements for Schedule II prescriptions;
- Refills are not allowed on new HCP prescriptions;
- Prescriptions for HCPs may be written on a hard copy, original prescription or received by electronic transmission, where allowed. Receipt by fax will not be allowed;
- Pharmacies must use a DEA Form 222 to purchase HCPs from a distributor. Purchasing and stocking HCPs will require additional recordkeeping and security requirements;
- Prescriptions for HCPs that are issued before Oct. 6, 2014, that have authorized refills may be dispensed in accordance with DEA rules for refilling, partial filling, transferring and central filling Schedule III-V controlled substances until April 8, 2015. However, state law, insurance limitations, and some pharmacy quality and safety operations and processes may not allow for these prescriptions to be refilled. Prescribers should be prepared to provide a new hard copy or a new electronic prescription for patients after Oct. 6, 2014, rather than have patients use what would have been existing refills;
- Pharmacies may continue to dispense HCPs in commercial containers labeled as Schedule III controlled substances, rather than placing the medication in a prescription vial. However, the DEA requires all other commercial containers of HCPs to be labeled as Schedule II controlled substances (this applies to manufacturers and distributors);
- The DEA permits prescribers to issue multiple prescriptions authorizing a patient to receive a total of up to a 90-day supply of HCPs; and
- Phone-in refills for HCPs are no longer allowed except for emergency situations. In these emergency cases, a small supply of up to five days may be authorized for filling and dispensing until a new “hard copy” prescription can be provided to the pharmacy for the patient. The new prescription must be provided to the pharmacy within seven days of the phoned-in emergency prescription. The face of the prescription must state, “Authorization for Emergency Dispensing.”
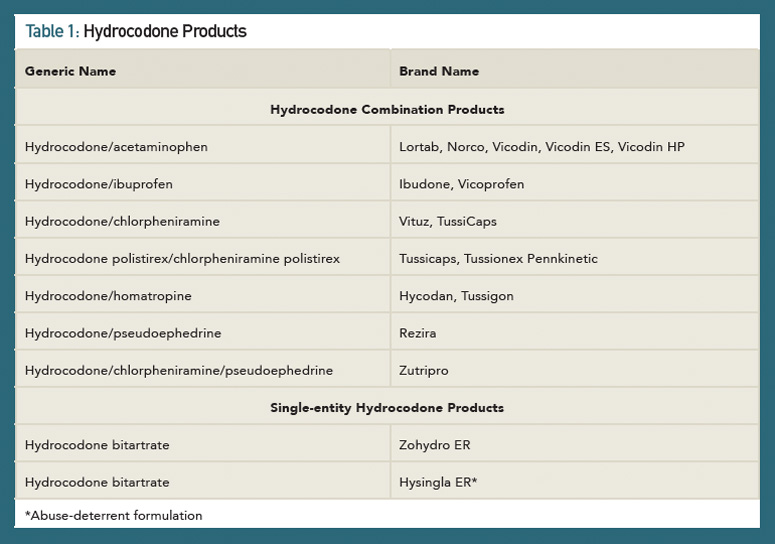
In 2012, the FDA approved a risk evaluation and mitigation strategy (REMS) for highly potent opioids, such as extended-release (ER) and long-acting (LA) medications.7,8 A major goal of opioid REMS programs was to reduce harm from prescription opioid misuse and abuse while continuing to provide access to these medications for patients’ pain management. Another strategy to achieve the goal of reducing harm from opioids was the development of abuse-deterrent formulations. Abuse-deterrent formulations are designed to reduce people’s ability to extract the active opioid ingredient from the dosage form. Individuals can try to do this by chewing the formulations and/or smashing them into a powder so they snort or inject the opioid. In late November (2014), the FDA approved hydrocodone bitartrate (Hysingla ER) as an “abuse-deterrent” tablet that cannot be easily crushed or chewed.9 The product forms a thick gel when crushed, making it difficult to inject. At the time of this writing, Table 1 lists the currently available HCPs and single-entity hydrocodone products.
New federal regulations will require additional planning to prevent disruption in workflow and to avoid gaps in pain management. Research gaps exist related to opioid efficacy and management, including lack of effectiveness studies on long-term benefits and harm of opioids for use in chronic non-cancer pain (CNCP).10 Patients on chronic opioid therapy should be managed according to best practices and universal precautions, such as screening for depression and not using concomitant sedative-hypnotics or benzodiazepines.11 Strategies to provide optimal care to CNCP need to be balanced with efforts to mitigate opioid prescription abuse.
Brodalumab Drug Update
The monoclonal antibody, brodalumab, met its primary endpoints in a late-stage study in adult patients with moderate-to-severe plaque psoriasis compared with ustekinumab and placebo.12 Brodalumab targets an interleukin (IL) 17 receptor to inhibit inflammatory signaling. The AMAGINE-2 trial included more than 1,800 patients who were randomized to receive either brodalumab 140 mg, brodalumab 210 mg, ustekinumab or placebo every two weeks for 12 weeks. Patients in the brodalumab arms were then re-randomized to receive one of four different maintenance brodalumab regimens. PASI 100 was achieved in 44% of brodalumab 210 mg-treated patients, and 34% of patients in a prespecified weight-based group also achieved PASI 100, vs. 22% of ustekinumab-treated patients. PASI 75 scores were more comparable between the different groups. Brodalumab-treated patients (77–86%) achieved PASI 75, and 70% of ustekinumab-treated patients achieved PASI 75 vs. 8% of placebo-treated patients.
Michele B. Kaufman, PharmD, CGP, RPh, is a freelance medical writer based in New York City and a pharmacist at New York Presbyterian Lower Manhattan Hospital.
Mary Choy, PharmD, CGP, RPh, is an associate professor at the Touro College of Pharmacy in New York and a clinical pharmacist at Metropolitan Hospital in New York.
References
- Horton DB, Scott IV FI, Haynes K, et al. Antibiotic exposure and the development of juvenile idiopathic arthritis: A population-based case-control study. Arthritis Rheumatol. 2014;66(11):Suppl. Abstract 929.
- Sharma TS, Harrington TM, Olenginski TP. Aim for better gout control: A retrospective analysis of preventable hospital admissions for gout. Arthritis Rheumatol. 2014;66(11):Suppl. Abstract 2322.
- Goldfien R, Herrinton L Monitoring methotrexate and leflunomide treatment for liver toxicity: The Kaiser Permanente experience. Arthritis Rheumatol. 2014;66(11):Suppl. Abstract 1360.
- Panchal S, Flint J, van de Venne M, et al. A systematic analysis of the safety of prescribing anti-rheumatic immunosuppressive and biologic drugs in pregnant women. Arthritis Rheumatol. 2014;66(11):Suppl. Abstract 1358.
- National Survey on Drug Use and Health. U.S. Department of Health and Human Services. Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality. 2014 Sep. http://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.pdf.
- Drug Enforcement Administration. Schedules of Controlled Substances: Rescheduling of Hydrocodone Combination Products from Schedule III to Schedule II. 2014 Aug 22. http://www.regulations.gov/#!documentDetail;D=DEA-2014-0005-0588.
- FDA. Opioid drugs and risk evaluation and mitigation strategies (REMS). 2014 Oct 9. http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm163647.htm.
- FDA. List of long-acting and extended-release opioid products required to have an opioid REMS. 2013 Apr 22. http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm251735.htm.
- FDA. FDA approves extended-release, single-entity hydrocodone product with abuse-deterrent properties. 2014 Nov 20. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm423977.htm.
- Chou R, Ballantyne JC, Fanciullo GJ, et al. Research gaps on use of opioids for chronic noncancer pain: Findings from a review of the evidence for an American Pain Society and American Academy of Pain Medicine Clinical Practice Guideline. J Pain. 2009;10:147–159.
- Franklin GM. Opioids for chronic noncancer pain: A position paper of the American Academy of Neurology. Neurology. 2014;83(14):1277–1284.
- Barber J. Amgen, AstraZeneca’s brodalumab meets primary endpoints of third Phase III trial in moderate to severe plaque psoriasis. 2014 Nov 25. http://www.firstwordpharma.com/node/1248329?tsid=33&tsid=17#axzz3KDqIyQjQ.


