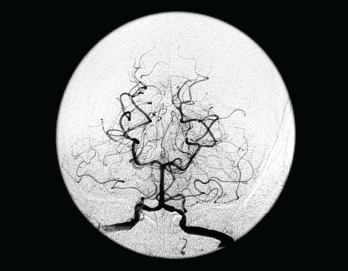
This frontal view from a vertebral angiogram shows the typical appearance of intracranial vasculitis.
Living Art Enterprises, LLC / Science Source
Many a rheumatology consult has centered on a perplexing question: Does this patient have central nervous system (CNS) vasculitis? At the 2021 ACR State-of-the-Art Clinical Symposium, Rula Hajj-Ali, MD, FACP, professor of medicine and associate director of vasculitis care and research, Cleveland Clinic Lerner College of Medicine, discussed this topic in detail, providing a series of clinical pearls that can be helpful in answering this query.
CNS vasculitis can be a primary process or secondary to an underlying condition. Although this entity is rare and diagnosis is often inferential, given the relative inaccessibility of CNS tissue for biopsy, many forms of the condition are treatable if detected early. Dr. Hajj-Ali noted CNS vasculitis can be seen in the context of systemic vasculitides, such as granulomatosis with polyangiitis (GPA), eosiniophilic granulomatosis with polyangiitis (EGPA), Behçet’s disease, giant cell arteritis and Takayasu arteritis. CNS vasculitis can also be associated with such conditions as common variable immunodeficiency (CVID) and a newly recognized genetic disease, deficiency of enzyme adenosine deaminase 2 (DADA2).

