Extensive diagnostic testing was performed. Notable findings included normal renal function; elevated alkaline phosphatase at 125 U/L (reference range [RR]: 9–122 U/L) with normal bilirubin, AST and ALT; leukocytosis with 17.9×103 cells/μL white blood cells (WBC; RR: 4.0–11.0×103 cells/μL); and neutrophilia with absolute neutrophil count of 13.24×103 cells/μL (RR: 2.00–7.60×103 cells/μL); mild anemia with hemoglobin of 12.4 g/dL (RR: 13.2–17.1 g/dL); thrombocytosis with platelet count of 498×103 cells/μL (RR: 150–420×103 cells/μL); and elevated, high-sensitivity C-reactive protein of 234.5 mg/L; normal procalcitonin and elevated antistreptolysin O (ASO) titer of 959 IU/mL (RR: ≤200 IU/mL).
Tests were negative for COVID-19, group A Streptococcus, urine chlamydia and gonorrhea, syphilis, QuantiFERON, Lyme antibody, Rickettsia IgG and IgM, hepatitis B surface antigen, hepatitis B total core antibody, hepatitis C antibody and human immunodeficiency virus. Parvovirus DNA was not detected by polymerase chain reaction (PCR). Blood cultures failed to identify a pathogen.
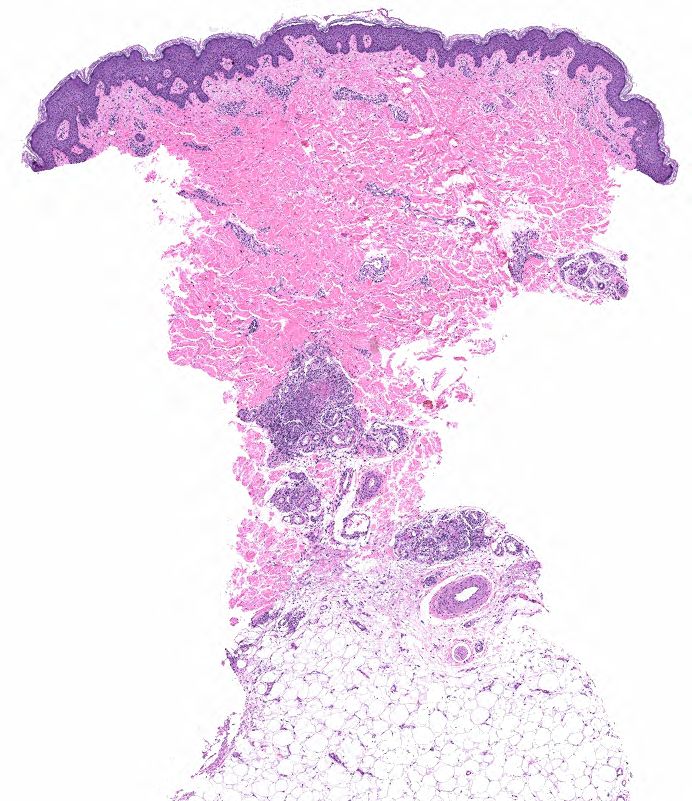
FIGURE 2A: Punch biopsy demonstrates an uninvolved epidermis with focal mid to deep dermal vasculocentric inflammation (H&E stain, 2x). (Click to enlarge.)
Rheumatoid factor was mildly positive at 17 IU/mL (RR: <14 IU/mL); antinuclear antibody (ANA) was 1:80, dense and fine speckled (RR: <1:80); angiotensin-converting enzyme (ACE) was normal. ANCA, myeloperoxidase antibodies (MPO), proteinase 3 (PR3) and cryoglobulin tests were negative. C3 and C4 were normal. Urinalysis returned 1+ protein and 1+ ketones; urine protein/creatinine was 0.10 mg/1.0 mg (RR: <0.10 mg/1.0 mg). Serum protein electrophoresis was normal, and serum free
kappa/lambda was absent.
Chest X-ray and transthoracic echocardiogram were unrevealing.
Left knee joint aspiration yielded turbid, yellow synovial fluid, with 10,301 nucleated cells/μL (RR: ≥2,000 nucleated cells/μL is classified as inflammatory synovial fluid), less than 3,000 red blood cells and no crystals. Synovial fluid culture did not yield an organism.