Both our studies were limited by their cross-sectional design and inherent inability to establish causality rather than document associations. Single determinations of inflammatory markers may not accurately represent concentrations over time and the cumulative burden of exposure. In addition, we were unable to precisely quantify lifetime dosages of medications to examine more fully and accurately the impact of pharmacologic therapy on the development of atherosclerosis.
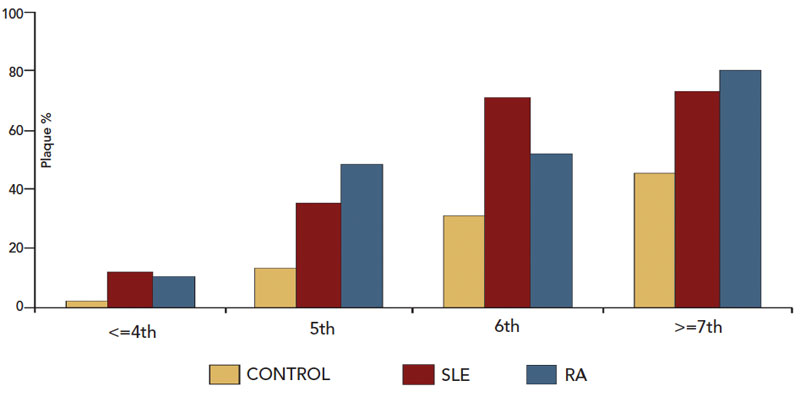
Although we did not identify a biomarker for atherosclerosis in our patients, we demonstrated an excess of preclinical atherosclerosis in RA and SLE compared to a matched control group, an increase that was most striking in younger individuals. Traditional ASCVD risk factors were not primarily responsible for accelerated atherosclerosis, and corticosteroid therapy was certainly not an atherogenic factor in these patients.
Take Control of Cardiac Risk Management
The evidence for accelerated atherosclerosis in SLE and RA is compelling, yet studies show that rheumatologists are not adequately implementing preventive strategies.19,20 In our study, RA patients with plaque had a mean total cholesterol value of 226 mg/dL, but therapy with lipid-lowering agents was uncommon (approximately 5%).

