(click for larger image)
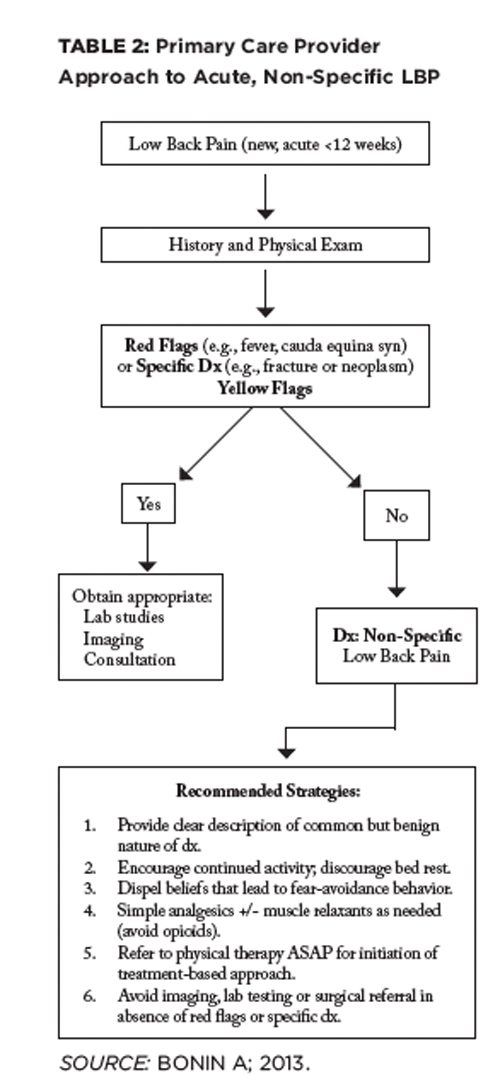
TABLE 2: Primary Care Provider Approach to Acute, Non-Specific LBP
TBC Category 2: Stabilization Subgroup
Spinal instability is considered one of the important causes of low back pain, but is poorly defined and not well understood. Core stabilization exercises have become extremely popular for those with LBP, but are not the solution for all categories of LBP. This subgroup has to be identified primarily through physical examination findings.
Typically, this patient reports a “catching” sensation in the lumbar spine with change of trunk position (e.g., sit to stand, sit to lying). The examiner may also find aberrant movements during flexion/extension. For example, the patient cannot return to an erect position from flexion without use of hands on thighs (thigh walking).
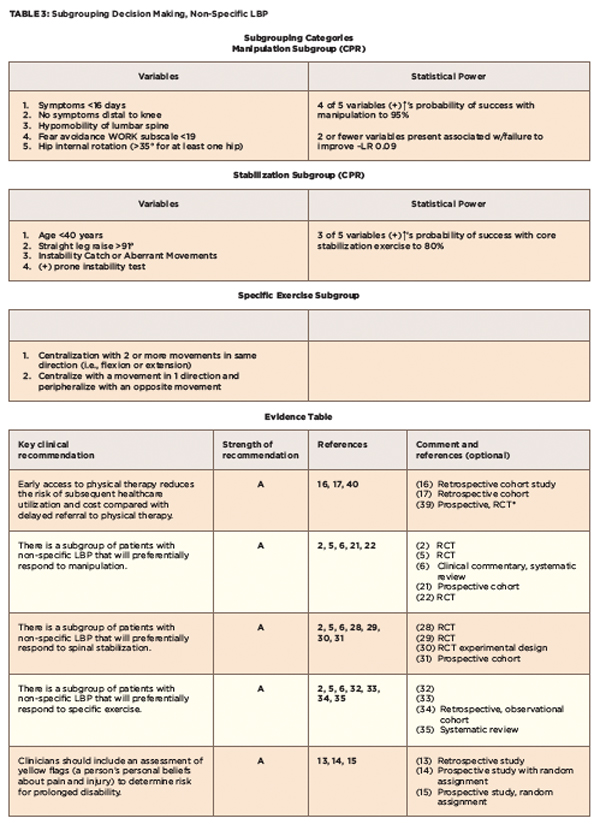
Hicks et al identified four factors that were predictive of improvement with spinal stabilization exercises (see Tables 3, and 4).31 A preliminary clinical prediction rule was defined as positive when at least three of these factors were present; the predictive accuracy of the stabilization CPR increases the probability of success with stabilization to 80%.31
TBC Category 3: Specific Exercise Classification
(click for larger image)
TABLE 3: Subgrouping Decision Making, Non-Specific LBP
This group is expected to respond preferentially to repeated end-range movements in a specific direction (flexion, extension or lateral shift). The existence of subgroups that comprise this group has been popularized by McKenzie.32 The hallmark examination criteria used in identifying patients for specific exercise is the “centralization phenomenon” (see Table 4).33,34 This involves the movement of pain from a more distal to a more proximal location. The movement producing centralization of radicular symptoms determines the directional preference (see Table 4).35,36 It is possible to have a directional preference without experiencing centralization of symptoms when a more comfortable position is experienced. The basic premise advocated for treating patients in a specific exercise classification is to use repeated end-range movements in the direction that caused centralization or diminished pain.
