The directions that patients may show a preference for are extension, flexion and lateral shift. Extension is the most common direction used; these responders tend to be younger in age and present with acute symptoms.6,35,36 The flexion-specific subgroup appears to be less common and most likely occurs in patients who are older and, often, with a medical diagnosis of lumbar spinal stenosis.6,36 The third movement direction classification is a lateral shift, which is considerably less common than flexion or extension categories and may represent more complex anatomic or functional situations.35,36
TBC Category 4: Traction Classification
Patients matched to this group are expected to have radicular symptoms, signs of nerve root compression and the absence of centralization with movement testing. The use of mechanical traction in the management of patients with acute or chronic LBP has generally not been endorsed by evidence-based practice.37,38 However, Fritz et al have provided some support for this approach in a randomized controlled trial that identified a subgroup of patients who are likely to respond to traction. Results of this study suggest this subgroup is characterized by the presence of leg symptoms and signs of nerve root compression, but also either peripheralization with extension movements or a positive crossed straight leg raise test.39
(click for larger image)
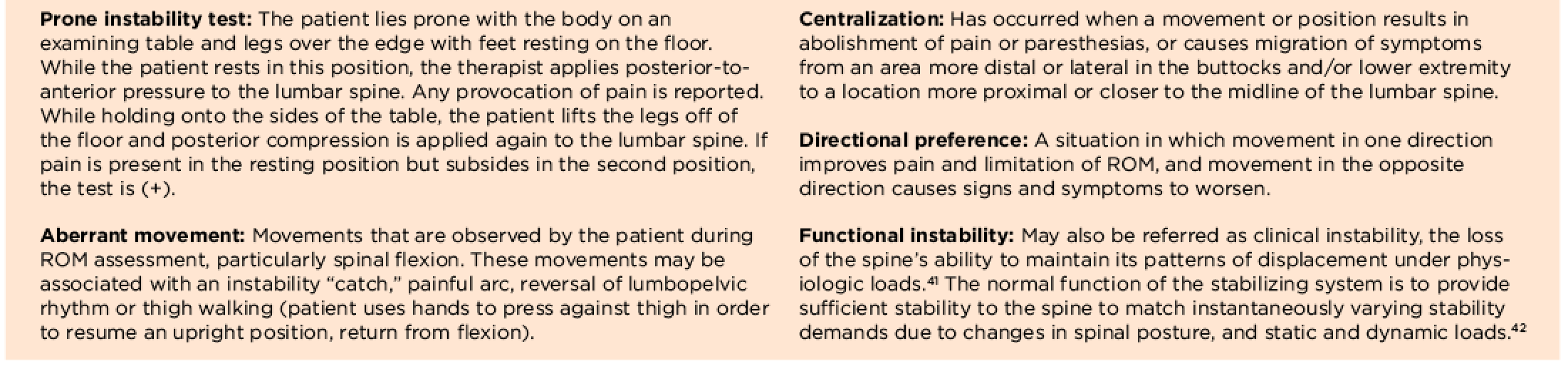
TABLE 4: Special Test & Definitions
Additional research is needed to further define this subgroup of traction responders, as well as studies to define parameters that will maximize any treatment effect (e.g., traction force, duration and patient position).
Final Comments
The majority of patients presenting with LBP cannot be diagnosed with a specific etiology, thus falling into the category of non-specific low back pain. When considering the rising cost of managing LBP and the attendant levels of disability, we can no longer afford to drive treatment decisions based on ineffective traditional approaches.
The treatment-based classification described above is a viable option that may assist practitioners in categorizing patients into better defined subgroups with recommended treatments likely to improve outcomes. Subgrouping patients with non-specific LBP, as well as early access to physical therapy, appears to be a more effective way to manage this most challenging condition.
 Emma W. White, PT, DPT, OCS, is an assistant professor at Winston-Salem State University-Department of Physical Therapy, N.C. Prior to this academic appointment, she owned and managed an orthopedic outpatient physical therapy practice, Thomasville Physical Therapy (October 1991–April 2008). Dr. White has more than 30 years of clinical practice experience. She received her physical therapy degree from the Medical College of Virginia in 1978 and a doctorate degree in physical therapy from the University of North Carolina at Chapel Hill in 2008.
Emma W. White, PT, DPT, OCS, is an assistant professor at Winston-Salem State University-Department of Physical Therapy, N.C. Prior to this academic appointment, she owned and managed an orthopedic outpatient physical therapy practice, Thomasville Physical Therapy (October 1991–April 2008). Dr. White has more than 30 years of clinical practice experience. She received her physical therapy degree from the Medical College of Virginia in 1978 and a doctorate degree in physical therapy from the University of North Carolina at Chapel Hill in 2008.
