His symptoms, swelling and pain in his hands, wrists, ankles and toes, began nine days after he had a root canal and crown preparation. He went to an emergency department, where it was noted he had had a tick exposure. He was prescribed doxycycline and discharged.
Click to enlarge.
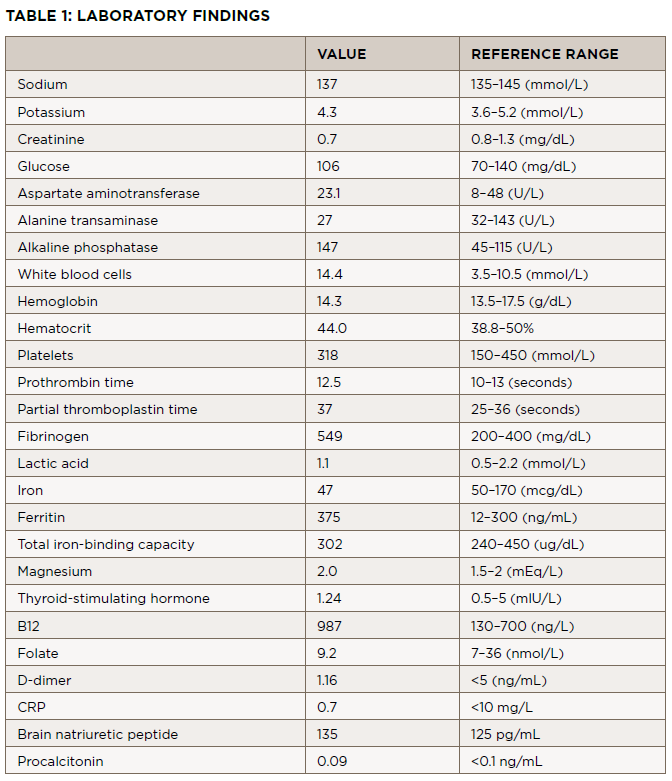
Two weeks later, he presented to the same emergency department with a fever of 103.4º and was admitted for suspected sepsis. He had an extensive evaluation, including blood cultures, a tickborne illness panel, computed tomography (CT) scans of his chest, neck, abdomen and pelvis, and transthoracic cardiac echocardiogram, which showed no acute abnormalities. Laboratory tests and results from that presentation are listed in Table 1.
Additional testing included:
- Serum protein electrophoresis (SPEP): consistent with acute phasereactant, faint restricted-band M spike migrating in the gamma-globulin region;
- Immunofixation: A faint band in IgG kappa could not be ruled out from the serum immunofixation pattern;
- Parvovirus B-19 IgM: negative at 0.1 (cutoff <0.9);
- Parvovirus B-19 IgG: elevated, positive at 4.3; (cutoff <0.9);
- Anti-neutrophilic cytoplasmic antibody (ANCA): negative;
- Hepatitis B and C naive by antibody testing;
- HIV: antibody negative;
- Parvovirus B19 IgM: negative, protein C: normal, protein S: normal;
- Factor 5 Leiden: normal;
- Lupus anticoagulant (dilute Russell viper venom time): 1.19 (cutoff <1.14);
- Anti-centromere antibody: negative;
- Anti-nuclear antibody (ANA): 1:80;
- Double-stranded DNA: negative;
- Rheumatoid factor: negative;
- anti-RNP and anti-Smith antibodies: negative;
- anti-Sjögren’s antibodies: negative;
- Cold agglutinins: negative;
- Urinalysis: normal;
- Legionella antigen: negative;
- Streptococcus pneumonia antigen: negative;
- Epstein Barr virus (EBV) nuclear antibody IgG: positive (cutoff >21.99);
- EBV capsid antibody IgM: negative;
- Cytomegalovirus (CMV) antibody IgM: negative;
- Anaplasma phagocytophilum DNA: not detected;
- Babesi microti DNA: not detected;
- Borrelia miyamotoi DNA: not detected;
- Ehrlichia chaffeensis DNA: negative;
- Lyme disease DNA: not detected.
He was seen by an infectious disease specialist who believed the patient had a viral illness. The patient was discharged.
