A 59-year-old woman presented to our rheumatology clinic with a six-month history of a symmetric polyarthritis. She initially experienced pain in both knees. As time progressed, she began to notice pain in her ankles, hips, shoulders, hands and feet. She experienced joint stiffness lasting for more than 30 minutes every morning. She also described worsening joint stiffness when she remained inactive for any length of time.
Corticosteroids had been prescribed for her in the past, and she said they did improve her pain by about 50%.
Her primary care provider had ordered lab tests. The test for rheumatoid factor was negative, but an anti-nuclear antibody (ANA) test was positive (nucleolar 1:160 and speckled 1:40).
The patient denied having any skin rashes, mucosal ulcers, renal abnormalities, cytopenias, alopecia, seizures, Raynaud’s phenomenon or thromboembolic events. Prior to the onset of her arthralgias, she denied any upper respiratory, urinary or diarrheal illnesses. She had not traveled outside the U.S.
Past medical history: The patient admitted to having smoked cigarettes in the past (half to a full pack daily for 15–20 years), but she had successfully quit 20 years before. She gave conflicting reports of prior chest X-rays; one of them had shown evidence of emphysema, and a more recent chest X-ray had not shown any lung pathology. There was no history of treatment for emphysema or other chronic pulmonary disease.
Physical exam: The patient’s oxygen saturation was normal, at 98% on room air. Her pulmonary exam was negative for rales, rhonchi and wheezing. Her abdominal exam was negative for tenderness, hepatosplenomegaly or a fluid wave. Upon examination of the extremities, she had clubbing involving all of the digits of her hands. She had swelling around the ankles bilaterally, but there was no palpable synovitis in any of her joints. Her lower legs were tender to palpation from the tibial plateau to the ankles, bilaterally.
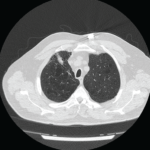
Due to the extent of her joint pain, X-rays of the hands, feet and knees were ordered for further evaluation. Rather than repeating a chest X-ray, which had provided conflicting information on two prior occasions, a computed tomography (CT) scan of the chest was ordered for further evaluation of an underlying pulmonary cause of her digital clubbing. Cardiac causes for her digital clubbing were deemed unlikely, because she had undergone a left heart catheterization in 2013 and no abnormalities were noted during the procedure. Further lab tests were obtained to evaluate her for an inflammatory arthritis.
She was started on 500 mg of nabumetone twice daily for pain control while she was undergoing further evaluation.
Findings: The patient’s comprehensive metabolic profile revealed a glucose level of 103 mg/dL (reference range [RR]: 65–99), urea nitrogen of 14 g/dL (RR: 7–25), creatinine of 0.74 g/dL (RR: 0.5–1.05), estimated glomerular filtration rate of 89 mL/min/1.73m2 (RR: ≥60), sodium 140 mmol/L (RR:135–146), potassium 4.4 mmol/L (RR: 3.5–5.3), chloride 108 mmol/L (RR: 98–110), calcium 8.7 mg/dL (RR: 8.6–10.4), globulin 2.4 g/dL (RR: 1.9–3.7), total bilirubin 0.3 mg/dL (RR: 0.2–1.2), alkaline phosphatase 129 U/L (RR: 33–130), aspartate transaminase 15 U/L (RR: 10–35), alanine aminotransferase 6 U/L (RR: 6–29), total protein 6.2 g/dL (RR: 6.1–8.1) and an albumin level of 3.8 g/dL (RR: 3.8–4.8).
The uric acid level was 5.4 mg/dL (RR: 2.5–7.0). The complete blood count showed a white blood cell count of 5.0 thousand/µL (RR: 3.8–10.8), hemoglobin 12.7 g/dL (RR: 11.7–15.5), hematocrit 38.9% (RR: 35–45) and a platelet count of 322 thousand/µL (RR: 140–400).