Vital signs in the emergency department were normal. An examination revealed a chronically ill-appearing man in no acute distress. He had multiple, erythematous, pearly nodules up to four centimeters in diameter on his left forehead, right eyebrow and left neck, suggestive of basal cell carcinoma (see Figure 1).
An erythematous maculopapular poikilodermic rash was present on his scalp, forehead, cheeks, neck, chest, upper back, upper arms, and dorsal aspects of his metacarpophalangeal and interphalangeal joints of his digits. He had painful periungual erythema of his fingernails.
His neurologic exam was notable for symmetric proximal weakness, with his upper extremities being weaker than his lower extremities. Manual muscle testing revealed the following Medical Research Council (MRC) grades: cervical flexion and extension 5/5, deltoids 2/5, biceps and triceps 3/5, wrist extensors and flexors 5/5 apart from 4+/5 left wrist extension, finger abduction 4+/5, finger flexion 5/5, hip flexion 3/5, quadriceps 5-/5, hamstrings 4+/5, anterior tibialis 5/5, gastrocnemius 5/5.
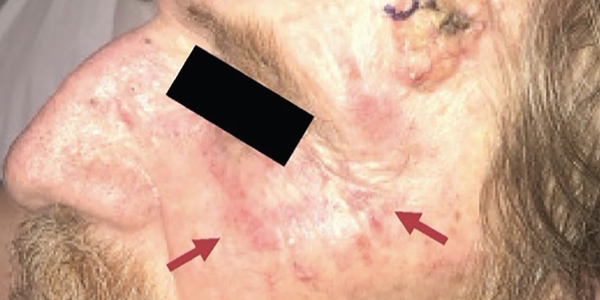
Figure 1. The physical examination revealed multiple, large, erythematous pearly nodules suggestive of basal cell carcinoma, as shown on his left temple, and a diffuse poikilodermic rash (maroon arrows).
He had no ocular, facial or bulbar weakness or sensory deficits. His deep tendon reflexes were trace at the biceps, brachioradialis and Achilles tendons. His patellar reflexes were 3+ with crossed adduction in both limbs. The remainder of the exam was unremarkable.
Emergency department laboratory testing from four weeks before was notable for normal renal function, normal blood counts, aspartate aminotransferase (AST) 313 IU/L (normal: 10–50 IU/L) and alanine aminotransferase (ALT) 124 IU/L (normal: 10–44 IU/L).
At follow-up with his primary care provider four days later, his liver transaminases were persistently elevated: AST 301 IU/L, ALT 134 IU/L and alkaline phosphatase (ALP) 116 U/L (normal: 40–129 U/L). Other abnormally elevated laboratory studies at this visit included C-reactive protein (CRP) 30 mg/L, anti-nuclear antibody (ANA) 1:320 with speckled pattern, anti-smooth muscle antibody (ASMA) 54 U, anti-mitochondrial antibody (AMA) 43.8 U, rheumatoid factor (RF) 57.8 IU/mL. Lyme IgG/IgM and Rocky Mountain Spotted Fever IgM screening tests fell within equivocal range.


