A contrast computerized tomography (CT) scan of his chest, abdomen and pelvis revealed numerous enlarged and heterogeneously enhancing mediastinal and right hilar lymph nodes (see Figure 2).
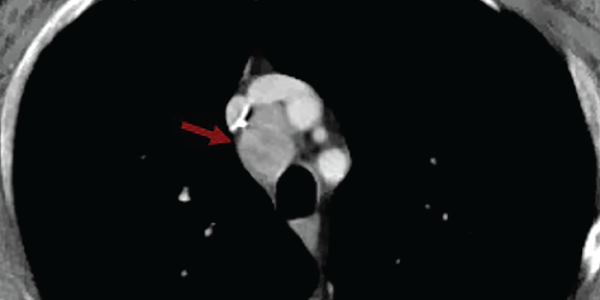
Figure 2. A contrasted CT scan of the chest shows numerous pathologic mediastinal and right hilar lymph nodes (maroon arrow).
Magnetic resonance imaging scan with myositis protocol of his lower extremities showed extensive symmetric T2 hyperintense signal involving the bilateral thigh and pelvis musculature with evidence of subcutaneous and perifascial edema consistent with myositis (see Figure 3).
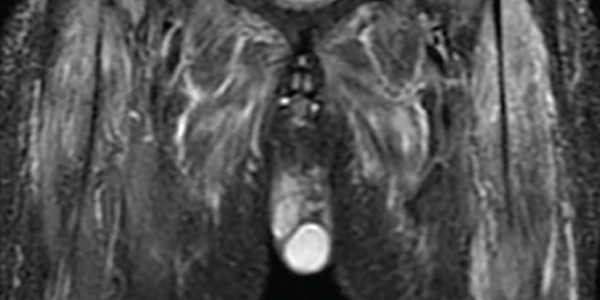
Figure 3. An MRI myositis protocol of the lower extremities with extensive, symmetric edema-like T2 signal of both thighs and the pelvis musculature.
Electromyography revealed abundant spontaneous activity in the form of fibrillation potentials and positive sharp waves in the deltoid and biceps brachii; it showed myopathic motor unit action potentials with early recruitment, consistent with an inflammatory myopathy.
A videofluoroscopic swallow study showed no oropharyngeal dysphagia. He underwent endobronchial ultrasound-guided fine needle aspiration biopsy of multiple lymph nodes. Rare tumor cells were present, with immunohistochemical testing positive for cytokeratin 7, suggestive of adenocarcinoma, and weakly positive for thyroid transcription factor 1, suggestive of a lung primary adenocarcinoma (see Figure 4).
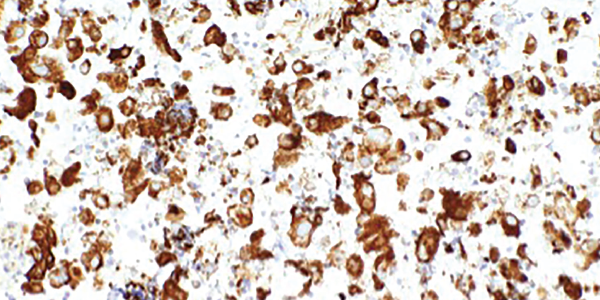
Figure 4. An ultrasound-guided, fine-needle aspiration biopsy of the mediastinal lymph nodes shows rare tumor cells. Immunohistochemical testing revealed the presence of cytokeratin 7 and thyroid transcription factor 1.
Next-generation sequencing was remarkable for missense mutations of NRAS, which are more commonly found in adenocarcinomas with a history of tobacco use, and TP53, which can be seen in a number of malignancies including lung cancers.2,3
Left forehead and right eyebrow lesion shave biopsies showed nodular and infiltrative pattern basal cell carcinoma, respectively. A right deltoid muscle biopsy demonstrated myopathic changes, fiber necrosis, fiber atrophy and minimal inflammatory cells, with no evidence of hemorrhage, granulomas or vasculitis (see Figure 5).


