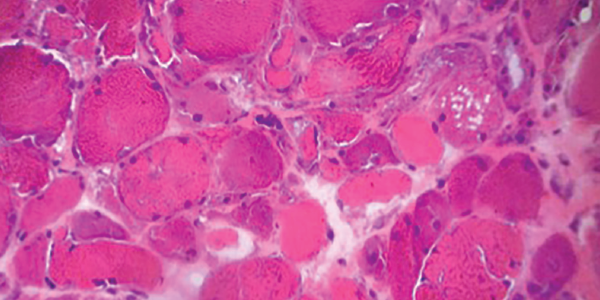
Figure 5. H&E staining of a muscle biopsy demonstrates myopathic changes, fiber necrosis and fiber atrophy, albeit a paucity of inflammatory cells.
MHC-I immunohistochemical staining showed patchy sarcolemmal up-regulation and an increased alkaline phosphatase staining pattern, consistent with an immune-mediated myopathic process. Electron microscopy of the muscle sample showed tubuloreticular inclusions (see Figure 6).
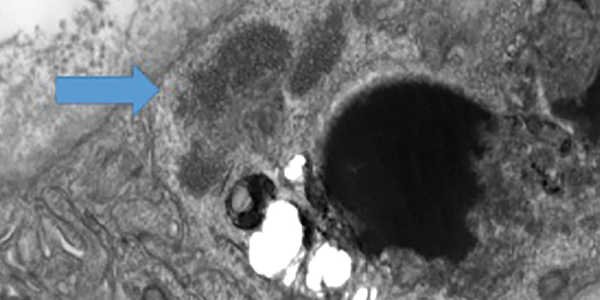
Figure 6 . Electron microscopy of a muscle biopsy shows tubuloreticular inclusions (blue arrow).
Our patient was diagnosed with dermatomyositis and began therapy with 1 mg/kg of oral prednisone daily on hospital day (HD) 2.


