Discussion
This is a case of anti-TIF1-γ positive paraneoplastic acute hemorrhagic dermatomyositis, an uncommon yet severe complication of dermatomyositis. As shown in Table 1, at least 16 adult cases of acute hemorrhagic dermatomyositis have been reported.4-18 The majority of these patients were middle aged, with approximately equal distribution among men and women.
Table 1
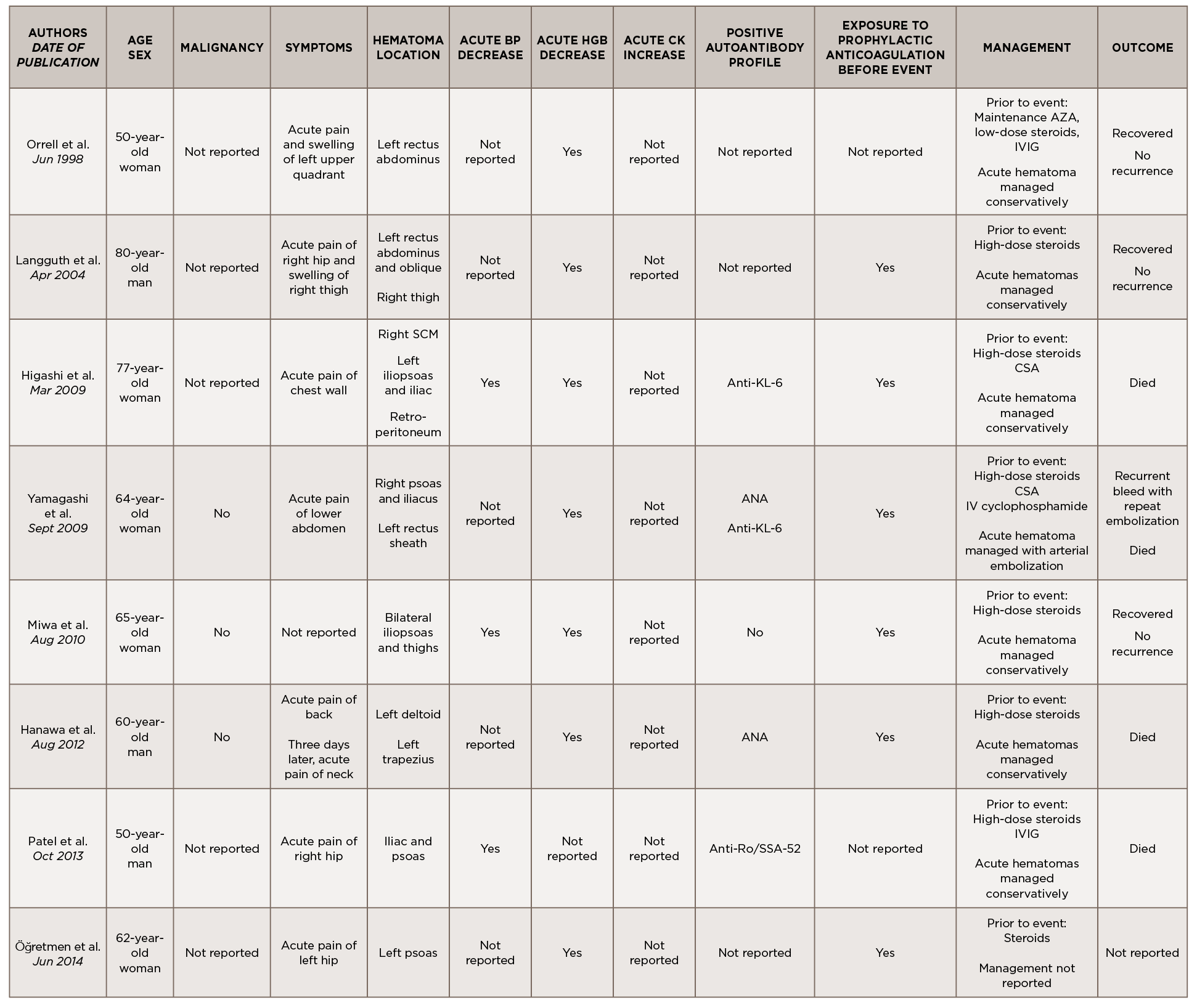
(Click for larger image) Table 1
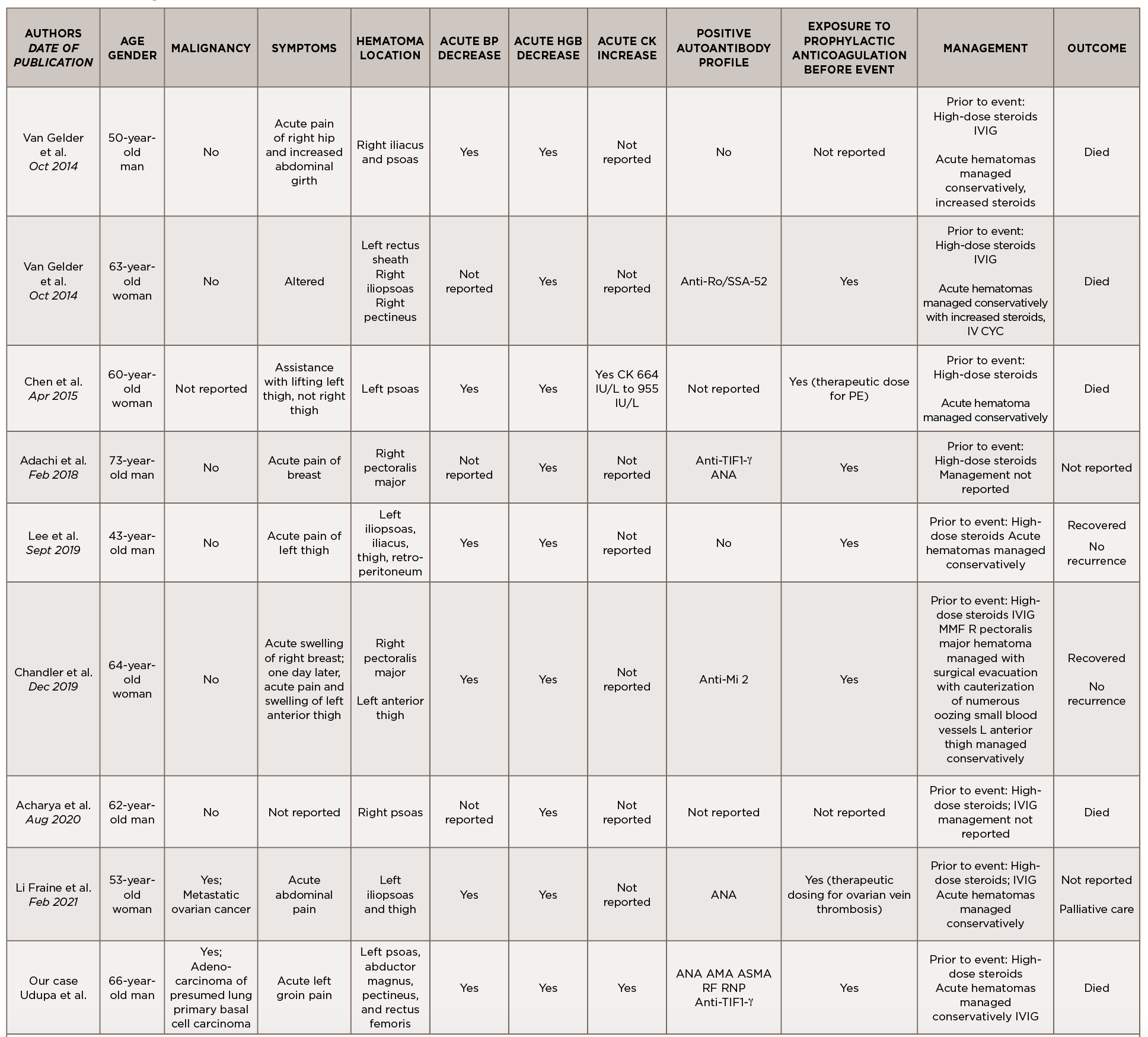
(Click for larger image) Table 1 continued from page
Legend: ANA, anti-nuclear antibody; AMA, anti-mitochondrial antibody; ASMA, anti-smooth muscle antibody; Anti-TIF1-γ, anti-transcription intermediary factor 1-γ; AZA, azathioprine; BP, blood pressure; CK, creatine kinase; CSA, cyclosporin A; CYC, cyclophosphamide; Hgb, hemoglobin; IVIG, intravenous immunoglobulin; MMF, mycophenolate mofetil; RF, rheumatoid factor; RNP, ribonucleoprotein; SCM, sternocleidomastoid; VS, vital signs
Although the past medical histories and clinical contexts differ slightly among these patients, only one was reported as having a concurrent malignancy.18 Most were newly diagnosed with dermatomyositis and subsequently developed atraumatic painful intramuscular hematomas, some of which were hemodynamically significant. All events occurred following administration of systemic glucocorticoids, and most events occurred following prophylactically or therapeutically dosed anticoagulation.
Some patients were treated with IVIG either before or after the hemorrhagic event, and a few were treated with disease-modifying anti-rheumatic drugs (DMARDs) either before, during or after acute hematoma formation.


