In addition to volitional control, diaphragmatic function is regulated by neuronal reflex arcs. Pleuralphrenic reflex arcs, activated by pleural afferents, lead to phrenic nerve inhibition. These arcs can be activated by pleural inflammation and thereby inhibit deep inspiration, resulting in chronic lung hypoinflation and decreased compliance.2-6 Similarly, pain-induced inactivation of the diaphragm may also play a role in diaphragm dysfunction in patients with shrinking lung syndrome.8
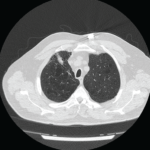
This case supports the theory that shrinking lung syndrome may arise as a complication of pleuritis because our patient had evidence both of pleural inflammation on CT scan and clear diaphragmatic dysfunction. No evidence supported structural causes of extrinsic restriction, such as chest wall deformities or pleural adhesions. No evidence of systemic myopathy was found given normal creatine kinase, and no other clinical features suggested myositis. Phrenic nerve stimulation tests were not attempted. Notably, Laroche et al. showed that a high proportion of SLE patients with shrinking lung syndrome had normal or approximately normal diaphragm contractility, suggesting that normal contractility is not enough to rule out a diagnosis of shrinking lung syndrome.9 Interestingly, even after resolution of all pleural inflammation and normalization of inflammatory markers, diaphragm dysfunction remained.
No evidence-based guidelines for the treatment of shrinking lung syndrome currently exist. Most commonly, patients are initially treated with corticosteroids. Adjunctive treatments include inhaled beta-2 agonists, theophylline, analgesia and chest physiotherapy. In steroid-refractory cases, additional immunosuppressants, such as azathioprine and cyclophosphamide, are used. Unfortunately, randomized clinical trials have not yet been undertaken to provide data regarding comparative efficacy. More recently, isolated case reports have documented a potential role rituximab, with or without cyclophosphamide.10-13
Overall prognosis for shrinking lung syndrome is variable. Most patients have improvement and stabilization of PFTs, and very few require supplemental oxygen. However, restrictive lung defects seen on PFTs rarely return to normal.6
In this case, in addition to PFTs, diaphragmatic ultrasound allowed monitoring of treatment response with a 50% improvement in diaphragm thickening after therapy with improving airflows.3 Despite the concerning clinical presentation and poor response to conventional therapy, it is thought that the low mortality rates of patients with shrinking lung syndrome may be secondary to the patient’s preserved ventilatory drive limiting further progression of respiratory deterioration, given the inflammatory process hypothetically causes a primarily functional process.7 However, this may also contribute to delayed diagnosis.
So far, our patient seems to match the typical progression of shrinking lung syndrome. Although her lung function has improved, she continues to have significant restrictive lung dysfunction.