Bangkok Click Studio / shutterstock.com
Lipoma arborescens is a rare, benign intra-articular lesion characterized by diffuse replacement of synovial tissue by mature adipocytes, causing a villous lipomatous proliferation of the synovial membrane.1 Typically, this is a monoarticular condition, with the knee being the most commonly affected although it has been rarely reported to occur in an oligo-/polyarticular fashion and in the subdeltoid bursa, glenohumeral joint, wrist, hip, elbow and ankles.2-6
The highest incidence of presentation occurs in the fourth and fifth decades of life.7 Originally, lipoma arborescens was thought to be more common in men, but recent studies indicate both sexes are affected equally.8
He reported that he had been having significant right knee pain for the past four days. The pain was constant, worsened with walking and improved with rest. The pain was associated with some weakness in his right lower leg. On questioning, the patient indicated that he had never had any major injury to the knee or recent trauma and that he had a history of intermittent right knee pain, although less severe than this current episode: He was admitted to the hospital several months before due to muscle cramping. He was diagnosed with a polyarticular acute gout flare and was subsequently treated with prednisone.
The patient reported some weight loss, but denied fevers, rashes, calf pain and pain in his other joints. A rheumatologist was consulted due to the patient’s history of gout.
On musculoskeletal exam, his knee was cool to the touch, with tenderness of the suprapatellar tendon and medial anserine bursa. Suprapatellar fullness was observed, and the patient had a limited range of motion of the joint, with pain disproportionate to the exam.
Laboratory testing demonstrated positive anti-nuclear antibody with a titer of 1:160 and normal complement levels. A glomerular basement membrane test was negative, as were tests for rheumatoid factor (RF) and anti-neutrophil cytoplasmic antibody. The erythrocyte sedimentation rate (ESR) was elevated to 74 mm/hr (reference range [RR]: 0–22 mm/hr for men), and the C-reactive protein was elevated to 40.1 mg/L (RR: <5–10 mg/L).
RF and anti-cyclic citrullinated peptide (CCP) antibody tests were negative during his previous admission.
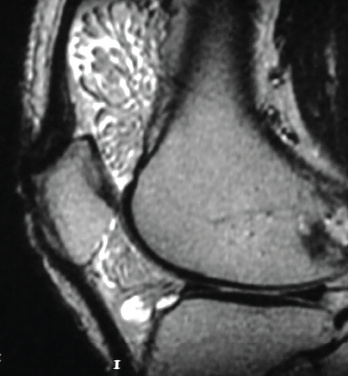
Figure 1. The MRI shows lipoma arborescens of the knee.
Given the minor swelling and the chronic, recurrent nature of the patient’s symptoms, joint aspiration and uric acid levels were deferred and imaging studies were ordered. An X-ray of his right knee demonstrated a small, suprapatellar joint effusion and nonspecific soft tissue swelling overlying the medial aspect of the knee, as well as edema within Hoffa’s fat pad, scattered vascular calcifications, mild narrowing of the medial compartment, mild subchondral sclerosis, minimal spurring of the tibial spines and no evidence of chondrocalcinosis.
At this point, a magnetic resonance imaging (MRI) scan of the knee was recommended. It demonstrated moderate joint effusion with lipoma arborescens (see Figure 1). A diagnosis of lipoma arborescens of the knee was made, and an orthopedic surgeon was called to further manage the patient.
The surgeon agreed with the diagnosis and administered a steroid injection into the joint for pain relief. Eventual joint replacement and synovectomy were scheduled, and the patient was discharged for follow-up.
Discussion
Given its uncommon nature, lipoma arborescens is rarely recognized as a potential cause of progressive and persistent joint swelling and pain. Diagnosis can be made with an MRI of the affected joint, sparing patients unnecessary examinations and procedures.
Johandi et al. demonstrate the utility of MRI in a similar clinical scenario involving a 51-year-old man presenting with unilateral knee pain and swelling and more than one year of misdiagnoses and unnecessary treatments.9 The patient described by Johandi et al. received plain radiographs at his initial visit and was subsequently diagnosed with degenerative osteoarthritis. He later presented with new-onset, bilateral, polyarticular arthritis of the wrist and metacarpophalangeal and proximal interphalangeal joints, in addition to persistent right knee pain and swelling. With normal lab findings and sterile fluid on knee joint aspiration, the patient’s diagnosis was changed to inflammatory oligoarthritis, and he was started on prednisolone and sulfasalazine therapy. Only after being referred to an orthopedic surgeon for synovectomy to rule out synovial tuberculosis was an MRI of the knee performed, which definitively pointed to a diagnosis of lipoma arborescens of the knee.
Given its uncommon nature, lipoma arborescens is rarely recognized as a potential cause of progressive & persistent joint swelling & pain.
Chronic joint pain and swelling can be challenging to diagnose and manage, and frustrating for patients experiencing the symptoms without a definitive solution. Both the above case presentation and the case described by Johandi et al. are complicated in that each patient had presented with a history of chronic polyarticular joint pain.
Supporting the hypothesis that lipoma arborescens is largely due to a reactive process, Vilanova et al. found that most patients present with symptoms suggestive of meniscopathy and are found to have degenerative joint changes and meniscal tear.8 Therefore, a reasonable degree of suspicion should be maintained for patients with such clinical signs and symptoms. Fortunately, the patient we have described was not exposed to unnecessary medical management, and diagnosis was made with MRI.
In Sum
The importance of including lipoma arborescens in the initial evaluation of patients with chronic, unremitting joint pain and swelling is demonstrated in the case above. A simple MRI provides a definitive diagnosis and synovectomy allows relief of patient symptoms. The etiology of this condition remains unknown; however, in many cases it is associated with such conditions as degenerative joint disease, popliteal cysts in approximately 20% of reported cases, diabetes mellitus, rheumatoid arthritis and psoriatic arthritis, suggesting the possibility of lipomatosis as the result of a reactive process.7,8,10 Primary disease is exceedingly uncommon.10
Patients often present with chronic and progressive joint swelling, limited range of motion and pain of the affected joint. Therefore, clinicians should be more suspicious of lipoma arborescens in patients with a presentation similar to the above case and a history consistent with degenerative joint disease, rheumatoid arthritis or other disease that could potentially fuel the reactive lipomatosis process.
Given the broad differential diagnosis, including pigmented villonodular synovitis, malignancy, synovial chondromatosis and rheumatoid arthritis, it is undoubtedly important to first rule out other rheumatic disease states and inflammatory arthropathies that can be acted upon. However, once initial diagnostics don’t provide an explanation for underlying symptomatology, clinicians should consider investigation with MRI; it is the gold standard for diagnosing lipoma arborescens.
In patients with this condition, an MRI will demonstrate a synovial mass of villous architecture depicting isointensity with subcutaneous fat. The mass is hyperintense on T1, but the signal is abolished in the sequences with fat saturation.11 There is no contrast uptake by the lesion, which excludes other inflammatory or neoplastic processes of the synovia.12 Therefore, MRI appearance of fatty synovial proliferation without other signal intensities within the lesion allows for a specific preoperative diagnosis.8
If the clinical picture is complicated and MRI does not shed light on the diagnosis, biopsy can be pursued. Histologic evaluation will show synovial hyperplasia and hypertrophy, with replacement of a significant amount of subsynovial tissue with mature adipocytes.8
The mainstay of treatment is synovectomy and, in primary disease, early intervention may be associated with decreased development of osteoarthritis.10,13 Current studies indicate a very low rate of recurrence.10
By acknowledging lipoma arborescens as a potential etiology of recurring joint pain and swelling, patients can be spared unnecessary diagnostics, empiric therapies and interventions aimed at managing more common arthropathies, and avoid progressive joint degeneration.13
 John Nawrocki, MD, completed an undergraduate degree in biology with a minor in biochemistry from Wilkes University, Wilkes-Barre, Pa., and medical school training at Geisinger Commonwealth School of Medicine, Scranton, Pa. His current research interests include immunology, hematology and oncology.
John Nawrocki, MD, completed an undergraduate degree in biology with a minor in biochemistry from Wilkes University, Wilkes-Barre, Pa., and medical school training at Geisinger Commonwealth School of Medicine, Scranton, Pa. His current research interests include immunology, hematology and oncology.
 Kevin Hess, DO, completed undergraduate degrees at Sacred Heart University, Fairfield, Conn., in cellular/molecular biology and biochemistry and his medical education at Rowan University School of Osteopathic Medicine, Stratford, N.J. He is a third-year internal medicine resident at ChristianaCare in Newark, Del. Current research interests include hematology and oncology.
Kevin Hess, DO, completed undergraduate degrees at Sacred Heart University, Fairfield, Conn., in cellular/molecular biology and biochemistry and his medical education at Rowan University School of Osteopathic Medicine, Stratford, N.J. He is a third-year internal medicine resident at ChristianaCare in Newark, Del. Current research interests include hematology and oncology.
Maryah Mansoor, MBBS, is a rheumatologist at Christiana Care Health System with special interest in scleroderma, lupus, myositis and ANCA-associated vasculitis.
Acknowledgment
We would like to thank the ChristianaCare Health System for allowing the opportunity to evaluate and treat this patient as we did in the case depicted above.
References
- Hallel T, Lew S, Bansal M. Villous lipomatous proliferation of the synovial membrane (lipoma arborescens). J Bone Joint Surg Am. 1988 Feb;70(2):264–270.
- Teusink M, El-Khoury G, Buckwalter J. Lipoma arborescens of the subdeltoid bursa: A case report. Iowa Orthop J. 2010; 30:177–178.
- Siva C, Brasington R, Totty W, et al. Synovial lipomatosis (lipoma arborescens) affecting multiple joints in a patient with congenital short bowel syndrome. J Rheumatol. 2002 May;29(5):1088–1092.
- Noel ER, Tebib JG, Dumontet C, et al. Synovial lipoma arborescens of the hip. Clin Rheumatol. 1987 Mar;6(1):92–96.
- Liddle A, Spicer D, Somashekar N, Chirag T. Lipoma arborescens of both knees: Case report and literature review. J Orthop Case Rep. Jul–Sep 2012;2(3):28–30.
- Ryu KN, Jaovisidha S, Schweitzer M, et al. MR imaging of lipoma arborescens of the knee joint. AJR Am J Roentgenol. 1996 Nov;167(5):1229–1232.
- Azzouz D, Tekaya R, Hamdi W, Montacer Kchir M. Lipoma arborescens of the knee. J Clin Rheumatol. 2008 Dec;14(6):370–372.
- Vilanova JC, Barceló J, Villalón M, et al. MR imaging of lipoma arborescens and the associated lesions. Skeletal Radiol. 2003 Sep;32(9):504–509.
- Johandi F, Chua Z, Malhotra R, Wang W. Knee pain: A cautionary tale of lipoma arborescens. BMJ Case Rep. 2016 Jun;2016:bcr2015214049.
- Yan CH, Wong JWK, Yip DKH. Bilateral knee lipoma arborescens: A case report. J Orthop Surg (Hong Kong). 2008 Apr; 16(1):107–110.
- Patil PB, Kamalapur MG, Joshi SK, et al. Lipoma arborescens of knee joint: Role of imaging. J Radiol Case Rep. 2011;5(11):17–25.
- Chaljub G, Johnson PR. In vivo MRI characteristics of lipoma arborescens utilizing fat suppression and contrast administration. J Comput Assist Tomogr. Jan–Feb 1996;20(1):85–87.
- Natera L, Gelber PE, Erquicia JI, Monllau JC. Primary lipoma arborescens of the knee may involve the development of early osteoarthritis if prompt synovectomy is not performed. J Orthop Traumatol. 2015 Mar;16(1):47–53.
Update June 3, 2022, to add the mentoring author, Dr. Mansoor.