Initial urinalysis several weeks prior to admission showed 2–3+ protein, 2+ blood, and no casts. Proteinuria was quantified with random urine-to-protein-creatinine ratio, which was elevated at 5.65 g/g Cr. The ANA titer was 1:640 in nuclear coarse speckled pattern; tests for anti-Smith and double-stranded DNA antibodies were negative.
Serum complements were not low. A test for phospholipase A2 receptor (PLA2R) antibody was negative. Tests for human immunodeficiency virus (HIV) antigen and antibody, hepatitis B surface antigen and antibody, and hepatitis C antibody were negative. A test for RPR was positive (1:256), with a positive confirmatory syphilis total antibody test. Chlamydia and gonorrhea polymerase chain reaction testing returned negative. Tests for anti-phospholipid antibodies were negative.
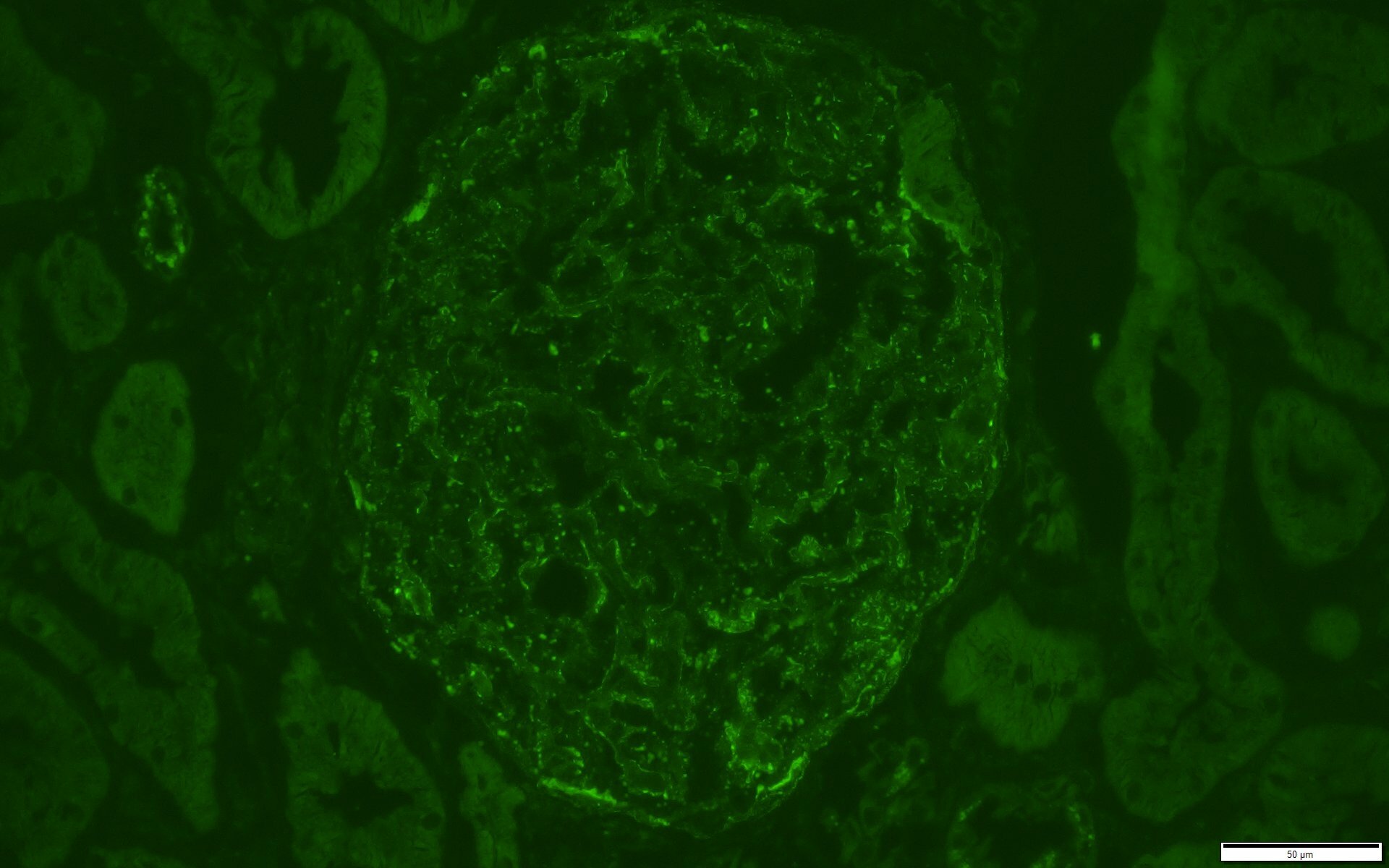
Figure 3: Immunofluorescence C1q Stain. Trace staining also noted for C1q in similar distribution as IgG stain. (Click to enlarge.)
The complete blood count test with differential was normal. Ferritin (408 ng/mL; RR: 12–300 ng/ mL for men) and erythrocyte sedimentation rate (ESR) (56 mm/ Hr; RR: 0–15 mm/Hr) were elevated; C-reactive protein (CRP) was just above the upper limit of normal (0.6 mg/dL; RR: <0.5 mg/dL).
Liver function tests revealed hypoalbuminemia (1.9 g/dL) and elevated alkaline phosphatase (413 U/L; RR: <129 U/L) and gamma-glutamyl transferase (872 U/L; RR: <61 U/L). Serum parvovirus B19 IgG (1.16 IV; RR: <0.90 IV) and IgM (1.97 IV; RR: <0.90 IV) were consistent with recently acquired infection.
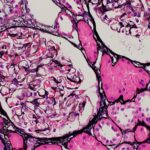
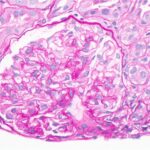
A renal biopsy was suggestive of classes II and V lupus nephritis; however, no crescents were identified (see Figure 1). Renal biopsy showed a combined (segmental) membranous and minimal mesangial pattern of glomerulonephritis with negative PLA2R antibody stain (see Figure 2). On immunofluorescence, glomeruli showed segmental, capillary loop and full-house pattern (positive for IgG, IgM, IgA, C3, C1q) co-staining (see Figures 3 and 4). Spirochete stain was negative on immunohistochemistry.
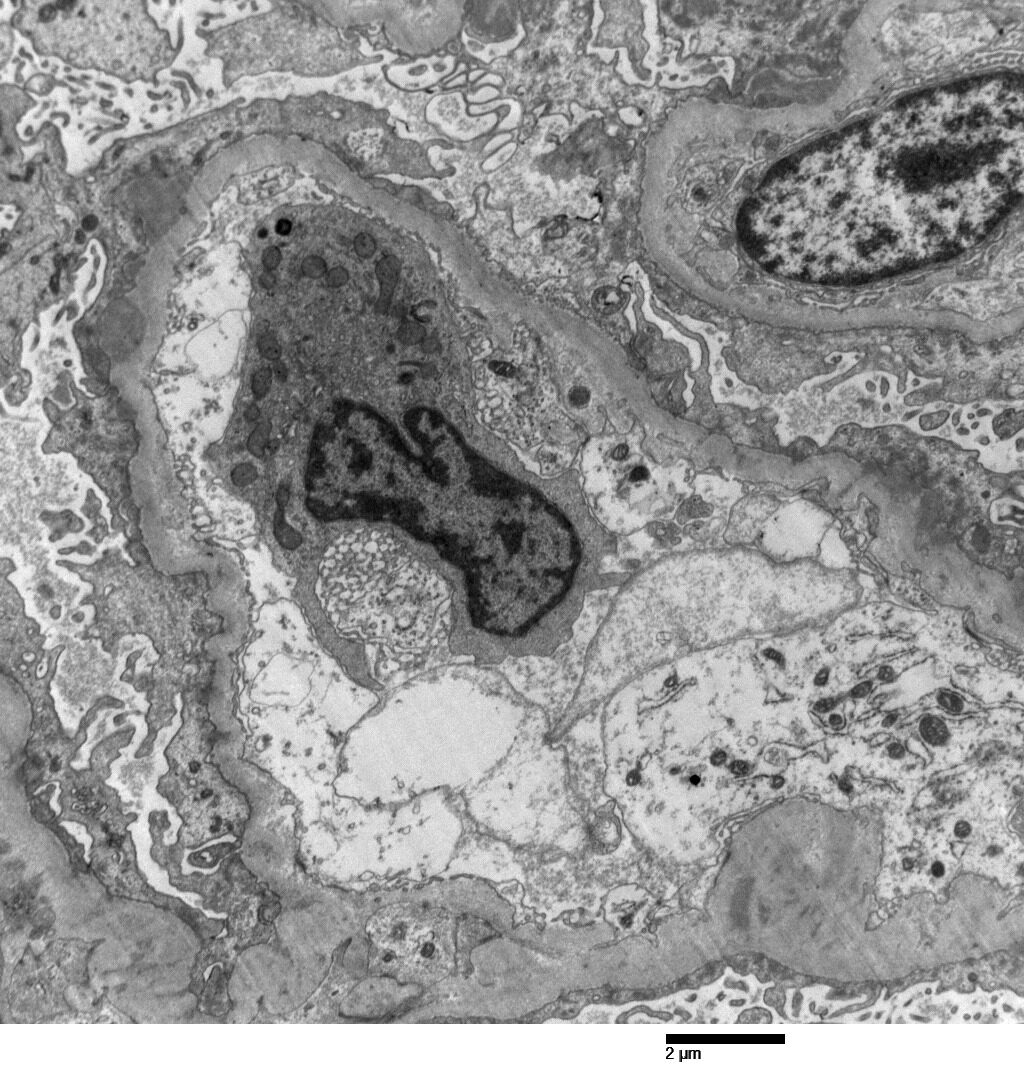
Figure 4: Electron Microscopy. Rare subepithelial and mesangial immune complex mediated type electron dense deposits present. Moderate podocyte epithelial foot process effacement. (Click to enlarge.)
Given the presence of persistent headache, along with neck tenderness and positive syphilis testing, a lumbar puncture with cerebrospinal fluid analysis was performed, which revealed normal cell count, negative gram stain, normal glucose and negative venereal disease research laboratory test.
Patient presented with nephrotic syndrome (i.e., nephrotic range: proteinuria, elevated cholesterol and edema), which improved during his hospitalization. He was treated with 30 mg of lisinopril daily and 40 mg of atorvastatin daily.