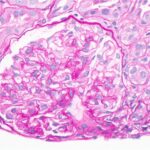
A renal biopsy was suggestive of classes II and V lupus nephritis; however, no crescents were identified (see Figure 1, opposite). Renal biopsy showed a combined (segmental) membranous and minimal mesangial pattern of glomerulonephritis with negative PLA2R antibody stain (see Figure 2, opposite). On immunofluorescence, glomeruli showed segmental, capillary loop and full-house pattern (positive for IgG, IgM, IgA, C3, C1q) co-staining (see Figures 3 and 4, this page). Spirochete stain was negative on immunohistochemistry.
Given the presence of persistent headache, along with neck tenderness and positive syphilis testing, a lumbar puncture with cerebrospinal fluid analysis was performed, which revealed normal cell count, negative gram stain, normal glucose and negative venereal disease research laboratory test.
Patient presented with nephrotic syndrome (i.e., nephrotic range: proteinuria, elevated cholesterol and edema), which improved during his hospitalization. He was treated with 30 mg of lisinopril daily and 40 mg of atorvastatin daily.
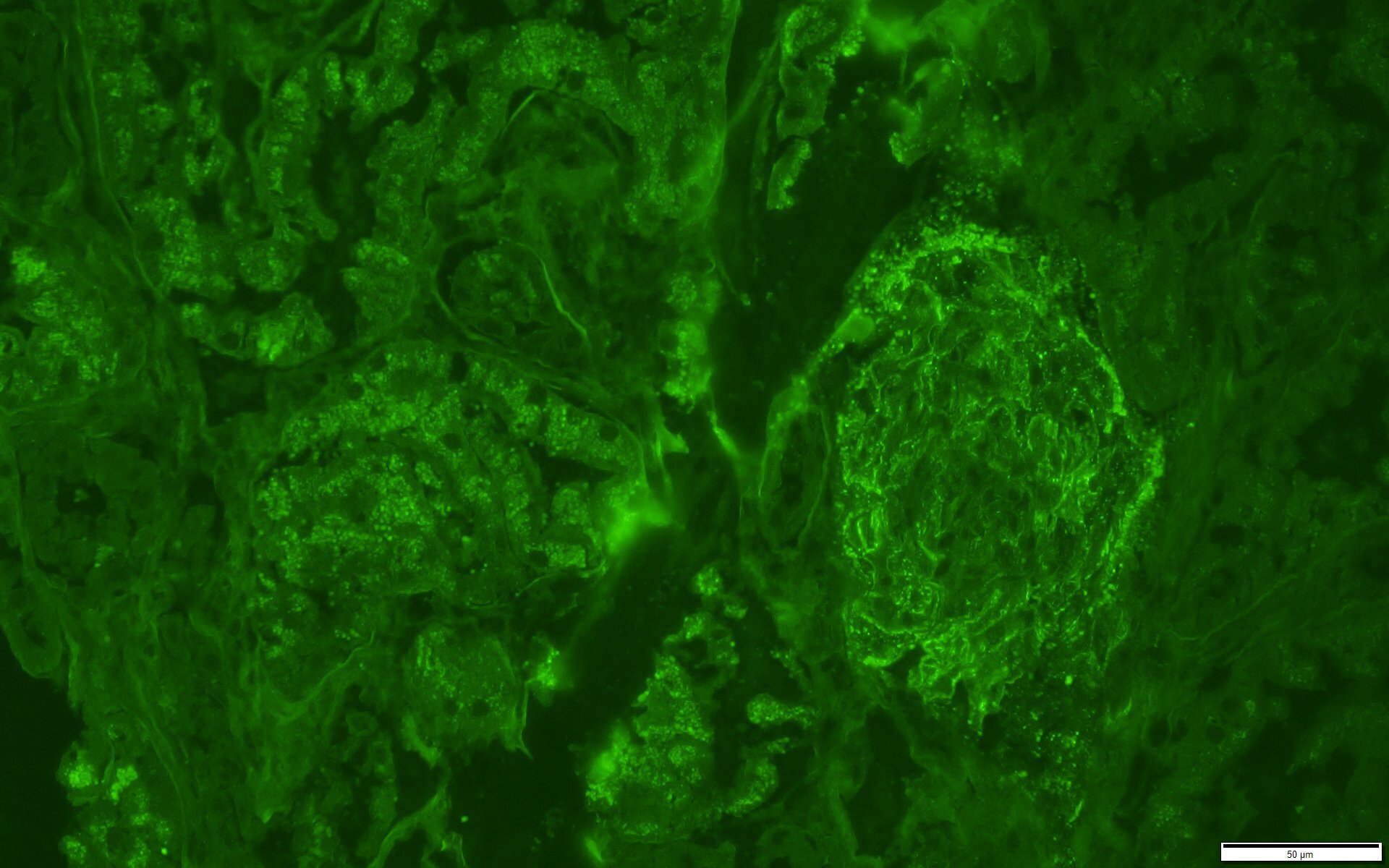
FIGURE 3: IMMUNOFLUORESCENCE IgG STAIN
IgG stain is positive in a granular pattern along capillary loop and rare mesangial areas.
(Click to enlarge.)
At his one-month outpatient follow-
up, his edema, headache, arthralgias, malaise, rash and diarrhea had all resolved. His cholesterol had normalized with statin therapy. Repeat urinalysis showed no blood and no protein, and the random urine-to-protein-creatine ratio had completely normalized (0.08 g/g Cr). His serum creatine declined to 1.2 mg/dL. His inflammatory markers had also completely normalized (ESR 1 and CRP <0.5 mg/dL), as had his alkaline phosphatase and albumin.
Discussion
Searching PubMed, we identified only one case of co-infection with syphilis and parvovirus B19 mimicking lupus nephropathy, as in our patient.1 Parvovirus B19 and especially syphilis have been reported to cause the same histologic features of lupus nephritis—or so-called pseudo-lupus nephritis. Although the presence of C1q deposits is nearly pathognomonic for lupus nephritis, it can also be seen when parvovirus B19 causes kidney disease.1