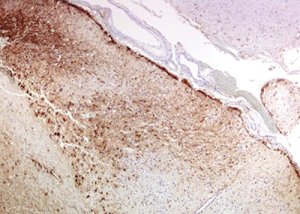
Figure 10: Immunohistochemistry for GFAP (glial fibrillary acidic protein) highlights the reactive gliosis of the subacute infarct.
The disease is considered in remission when the patient is stable and improved clinical and radiologic features are observed. Serial MRIs should be obtained to help in the assessment of disease activity, and clinicians may consider repeat CSF analysis.2
Efforts to limit accelerated atherosclerosis through aggressive control of diabetes, hypertension and dyslipidemia, as well as smoking cessation, is important. Routine vaccinations, osteoporosis prevention and prophylaxis for opportunistic infections should be included in treatment plan.2