The patient had taken levothyroxine and sertraline for several years. She had changed from triamterene-hydrochlorothiazide to metoprolol for blood pressure control about a year earlier.
Her symptoms did not improve with exercises or NSAIDs. Following a podiatry referral, the patient went to a rheumatologist.
The examination was significant for a positive, right Finkelstein maneuver, bilateral first MTP tenderness without swelling or erythema, bilateral greater trochanteric bursa tenderness, and a positive Patrick’s maneuver bilaterally.
A prior pelvic X-ray (see Figure 1) had shown sacroiliac joint osteoarthritis and enthesopathy, which, along with the examination findings, prompted the rheumatologist to order a pelvic MRI.
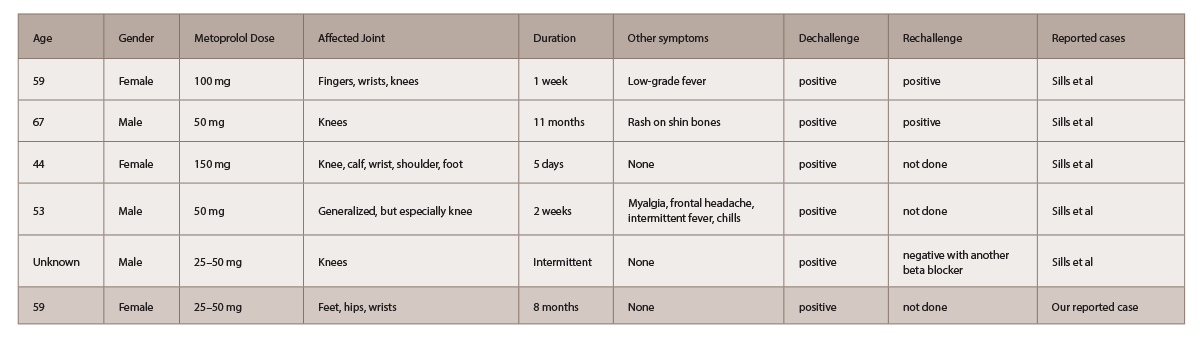
(click for larger image) Table 1: Five Cases of Self-Reported Metoprolol-Induced Arthralgias4
Further workup, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factory (RF), HLA B27, an ultrasound of the hand and wrist and the pelvic MRI were negative.
Metoprolol was discontinued upon the patient’s request while she was undergoing the workup, which resulted in complete resolution of her arthralgias within two to three days after drug cessation.
Discussion
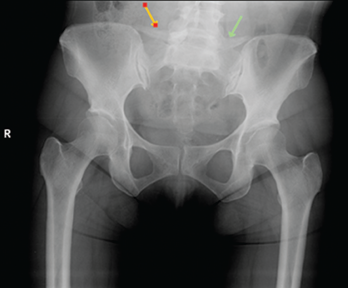
A pelvic X-ray had shown sacroiliac joint osteoarthritis and enthesopathy.