Click to enlarge.
During evaluation by his primary care doctor, his lab work demonstrated an elevated creatinine kinase, concerning for ongoing muscle damage, but the etiology of his symptoms was not identified.
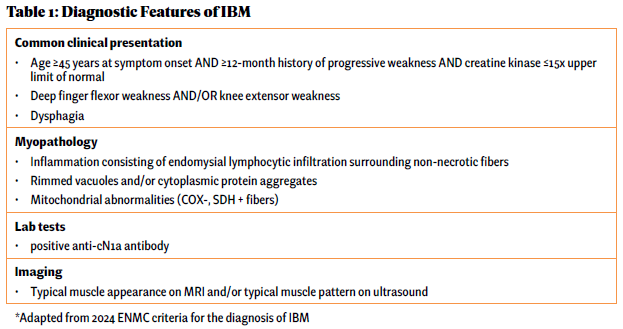
Over the next five years, he saw numerous specialists and underwent countless tests while his physical condition deteriorated. He underwent a muscle biopsy that was interpreted as polymyositis and was started on high-dose glucocorticoids for treatment. This failed to make an impact on his muscle strength. He was told not to exercise under the premise of causing further muscle damage, which likely exacerbated his weakness. Due to his progressive symptoms, he presented to the Johns Hopkins Myositis Center for a second opinion and was ultimately diagnosed with IBM based on his clinical history, muscle biopsy and physical exam (see Table 1 and Figures A, B & C).

FIGURE A: Finger flexor weakness in IBM.
By the time he was diagnosed, Mr. F had already experienced significant debility due to his disease and complications of futile high-dose glucocorticoid therapy, including weight gain, diabetes and gastrointestinal perforation.


