Here, we report a rare case of bilateral pulmonary artery stenosis secondary to GPA, underscoring the importance of recognizing large-vessel involvement as a potential manifestation of ANCA-associated vasculitis.
Case Presentation
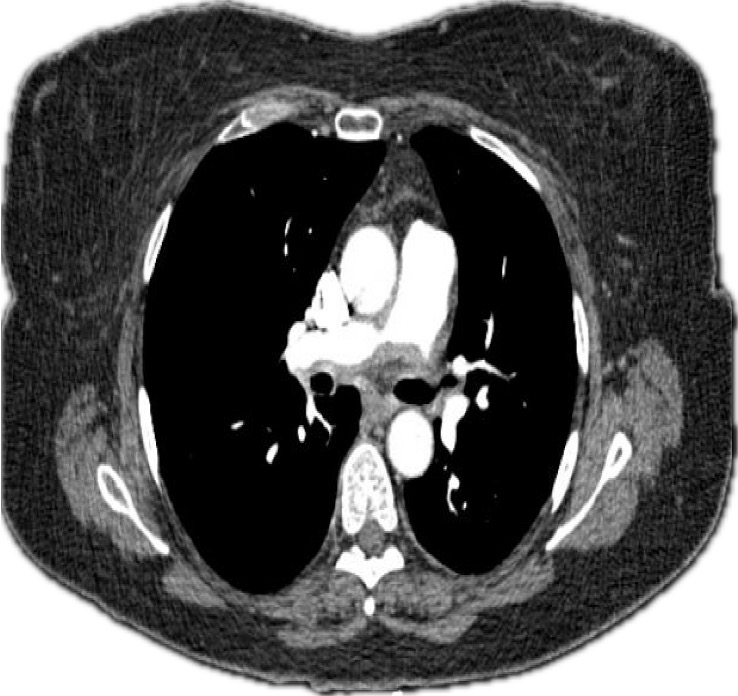
Figure 1: CTA of the chest showing stenosis of the right pulmonary artery. (Click to enlarge.)
A 62-year-old woman with a history of well-controlled type 2 diabetes mellitus presented with a progressive constellation of symptoms that began in early 2021. A nurse herself, initially she reported “hearing a bruit” in her chest without associated symptoms.
Around this time, she developed recurrent nasal congestion with bloody discharge and sinus infections. Over the ensuing months, she experienced progressive left-side hearing loss, recurrent otitis media requiring tympanoplasty and arthralgias. A few months later, she noted progressive bilateral leg swelling. Her physical therapist identified worsening exertional dyspnea and auscultated a heart murmur. She also experienced worsening fatigue and noted scattered petechiae on her legs, arms, and abdomen.
Given her worsening dyspnea, leg swelling and palpitations, she was referred to a cardiologist. A transthoracic echocardiogram revealed severe pulmonary hypertension with an estimated right ventricular systolic pressure (RVSP) of 102 mmHg, right ventricular dilation and a normal ejection fraction.
Holter monitoring ruled out arrhythmias. A computed tomography and angiogram (CTA) of the chest revealed ill-defined, soft-tissue thickening surrounding the right and left main pulmonary arteries, with moderate stenosis (see Figures 1 and 2).
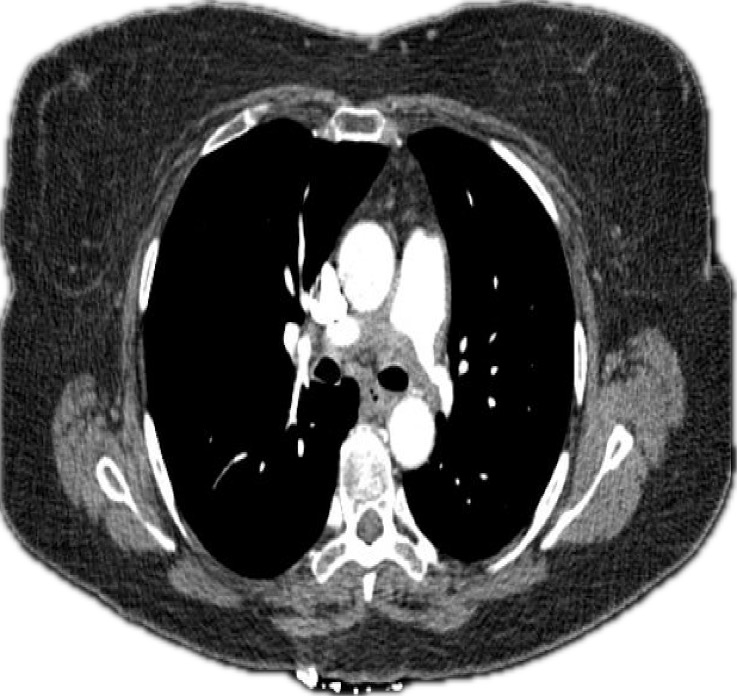
Figure 2: CTA of the chest showing stenosis of the left pulmonary artery.

