Her basic laboratory tests were unremarkable except for an anemia with a hemoglobin of 11.9 (reference 12.0–16.0 g/dL). A high-sensitivity C-reactive protein (hs-CRP) was 19 (reference <7.4 mg/L) with an erythrocyte sedimentation rate (ESR) of 5 (reference <25 mm/hr). A transesophageal echocardiogram revealed thickening of the ascending aorta, severe aortic insufficiency with a flail right cusp, aortic root dilation and thickening of the valve. Her left ventricular ejection fraction was 35%.
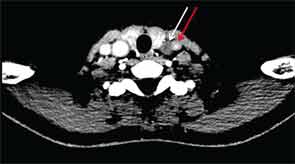
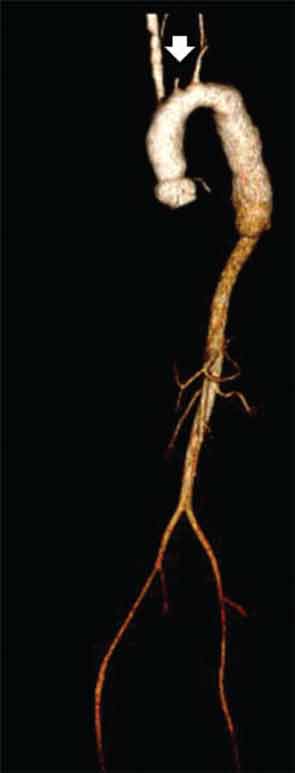
CT of the neck showed complete occlusion of left common carotid artery immediately above the stump (see Figure 1) and complete occlusion of the left internal carotid artery with retrograde filling via the circle of Willis. Significant wall thickening and multiple areas of irregularity and dilatation were seen in the right innominate, right common carotid and left subclavian arteries. A CT angiogram (CTA) of the chest, abdomen and pelvis demonstrated a dilated ascending and descending thoracic aorta with a maximum dimension of 4 cm with concentric wall thickening extending to the midthoracic aorta (see Figure 2). There was no involvement of her abdominal aorta.
The patient was given a pulse dose of glucocorticoids with methylprednisolone 500 mg intravenous daily for three days with improvement in the strength of her left brachial and radial pulses over the course of treatment. She was also initiated on aspirin 81 mg daily and azathioprine 50 mg daily, which was further titrated as an outpatient. After the glucocorticoid pulse, the dose was reduced to prednisone 1 mg/kg/day. Aortic valve replacement was deferred in order to treat the inflammatory vascular process and because she was well compensated clinically. She returned a month later and continued to have stable heart failure symptoms, although she had episodes of left-side amaurosis fugax, lasting less than 15 seconds. Her glucocorticoid dose will be tapered in anticipation of an aortic valve replacement.
Case 2
A 31-year-old Hispanic woman presented to the hospital with hypertension and renal failure.