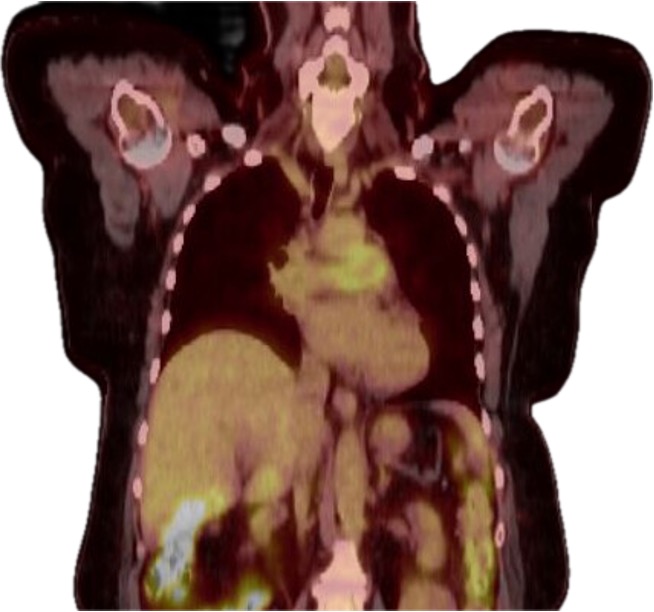
Figure 4 (coronal view): PET-CT demonstrating increased metabolic activity in the proximal pulmonary arteries. (Click to enlarge.)
We conducted a literature review using the following search terminology: (“Granulomatosis with Polyangiitis” [MeSH] OR “Microscopic Polyangiitis” [MeSH] OR “Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis” [MeSH] OR “ANCA-associated vasculitis” OR “Wegener’s granulomatosis” or myeloperoxidase antibody OR proteinase 3 antibody) AND (“Pulmonary Artery” [MeSH] OR “Pulmonary Artery Stenosis” [MeSH] OR “Pulmonary Arteritis” OR “pulmonary artery vasculitis”).
This search yielded 45 results, from which we reviewed eight relevant articles.2,4-10 Including our patient, we reviewed a total of nine patients.

