Polyarteritis nodosa (PAN) is a rare, necrotizing arteritis of the medium or small arteries that lacks the production of anti-neutrophil cytoplasmic antibodies (ANCA).1 PAN has a variety of clinical presentations and a spectrum of severity. Virtually any organ may be involved, and the disease can present with isolated or multisystem involvement. Greater than 90% of all patients experience constitutional symptoms at the time of diagnosis.2 Due to the variable presentation of the disease, the differential diagnosis for PAN is broad and includes infectious diseases, other systemic vasculitides, and vasculopathies, such as segmental arterial mediolysis (SAM) and vascular Ehlers-Danlos (vEDS).3,4
Case Presentations
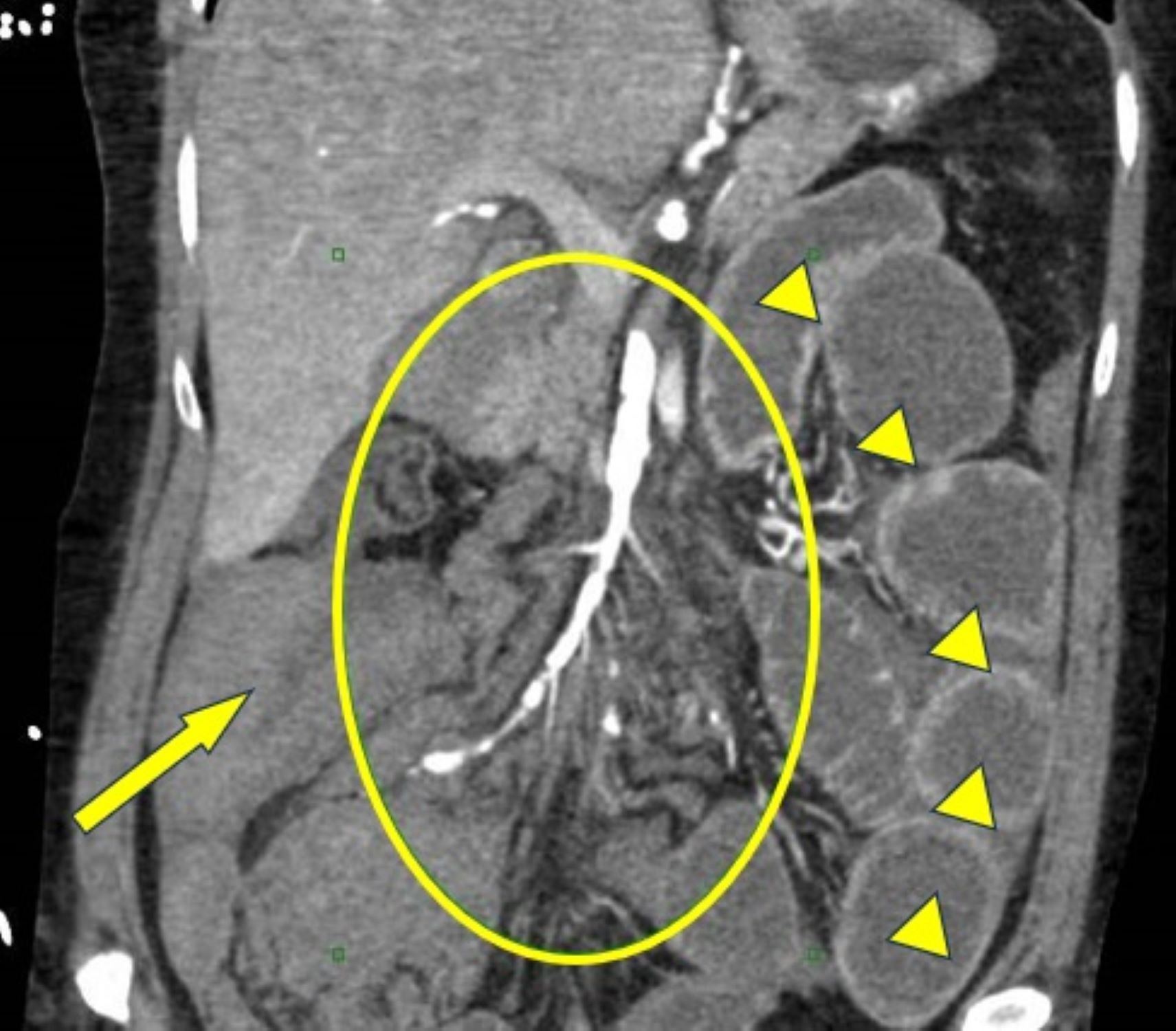
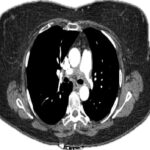
Figure 1. Sagittal section from CTA of the abdomen and pelvis taken on hospital day 12 highlighting SMA involvement in vED. The circle highlights the SMA diffuse irregularity and beading of the arterial wall. Arrowheads show hyperenhancement of the distal small bowel related to intestinal ischemia from distal SMA occlusions. The arrow points to hemoperitoneum. The patient also had dilation of the proximal small bowel with cutoff at the right lower quadrant anastomosis consistent with high-grade small bowel obstruction. (Click to enlarge.)
Case 1