Presentation
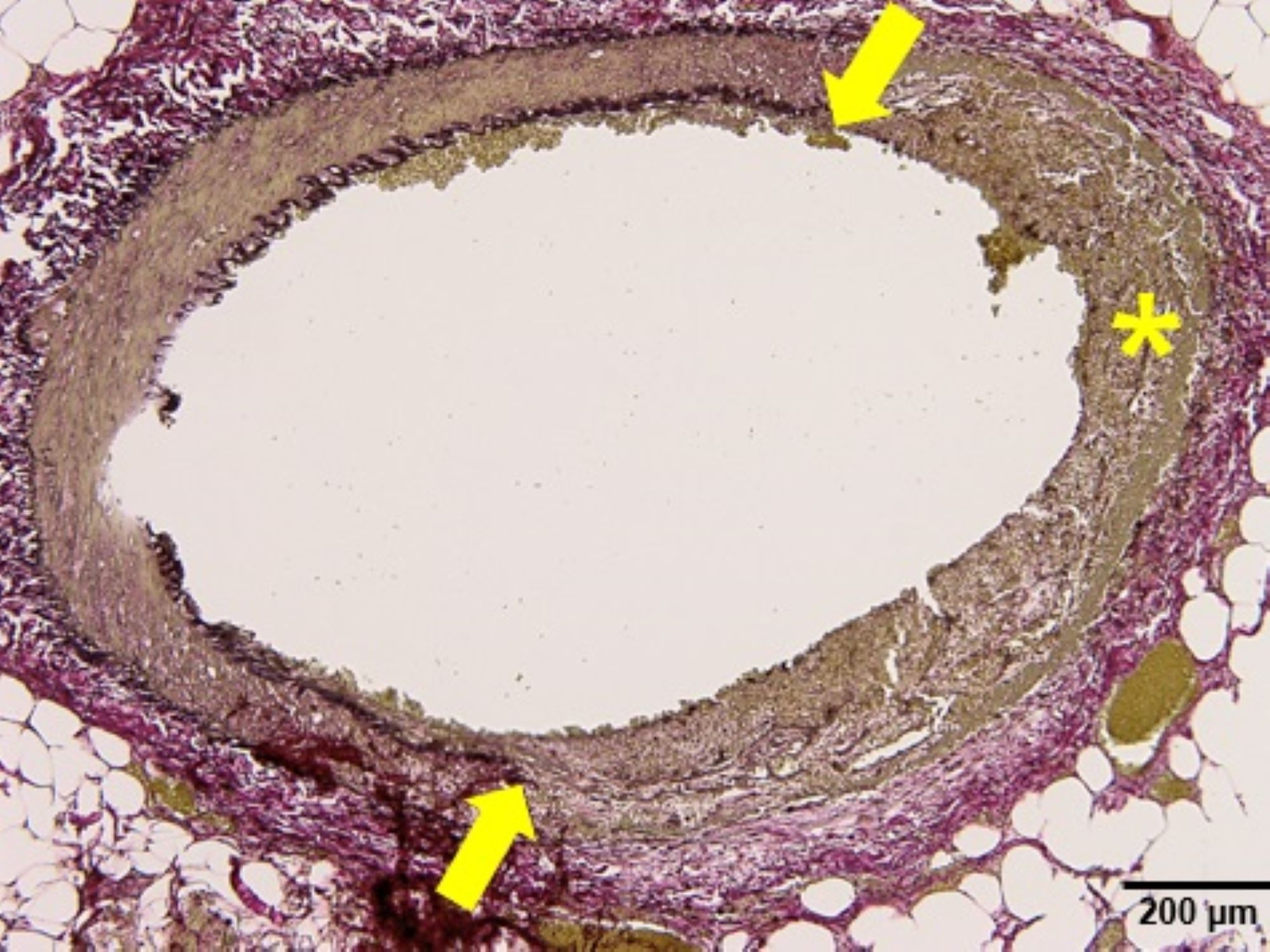
Figure 3b: The EVG special stain (x10 objective) highlights in another artery segmental necrosis of the arterial wall, including absence of both the external and internal elastic lamina, as indicated by the yellow arrows and asterisk. (Click to enlarge.)
Patients with SAM present with symptoms according to the affected vascular bed. The condition most commonly affects the splanchnic vessels, often leading to abdominal apoplexy due to aneurysmal rupture, or symptoms related to ischemia and infarction, as in our case.5,8,12 Less commonly, patients can present with hematuria or acute flank pain when the renal vasculature is involved.7,13–15 Additionally, isolated cases with histopathologic features compatible with SAM have been described in the coronary arteries of neonates, children and young adults, and the cerebral arteries of adults.5–7,16–20