Risk: The guidelines consider risk to the patient in determining the level of medical decision making—risk of significant complications, morbidity and mortality—and they recognize three gauges of this risk: the presenting problems, any diagnostic procedures you choose and any management options you choose. Key documentation principles to follow for this component are outlined in Table 1.
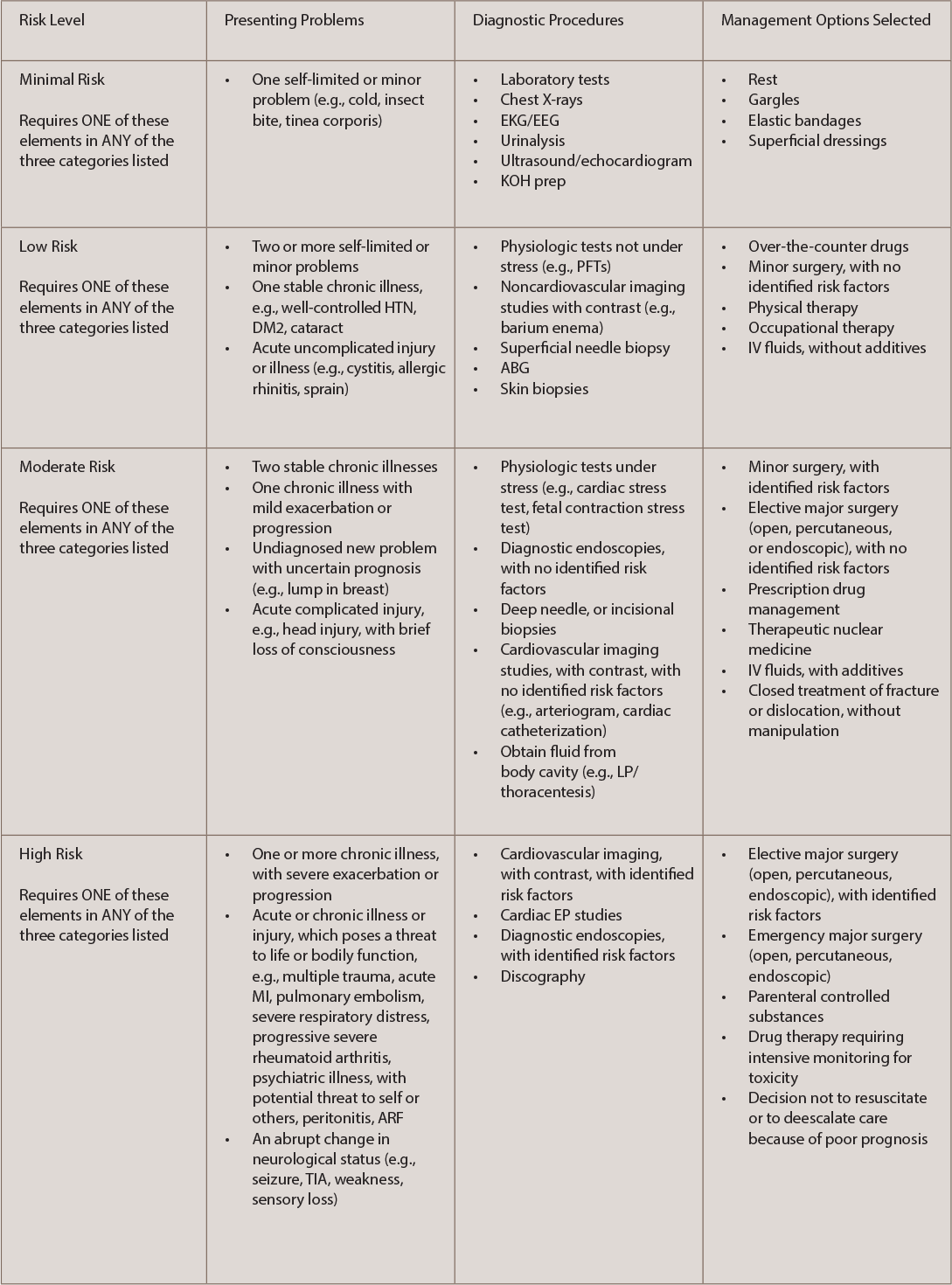
(click for larger image) TABLE 1: Key Risk Documentation Principles
The comprehensive process in medical decision making is an area that reflects evaluating, testing and treatment, and providers should take precaution to monitor practice improvement to avoid unnecessary audits and/or coding adjustments.