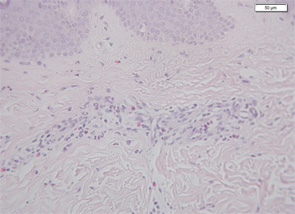
Therefore, a high level of suspicion and awareness is crucial in making the diagnosis of CAPS. There are several diagnostic aids to help diagnose these patients. These include a biopsy of the rash. Unlike classic urticaria, which is characterized by edema and the presence of mast cells, the rash in CAPS shows a dense neutrophilic infiltrate mainly in the lower (reticular) layer of the dermis, which tends to be perivascular and peri-eccrine (see Figure 5). Magnetic resonance imaging (MRI) of the brain with a focus on the inner ear often shows edema with gadolinium enhancement (occasionally also meningeal enhancement is present) (see Figure 6). Lumbar puncture during attacks may show increased opening pressure with pleocytosis and elevated protein levels. Hearing tests showing high-frequency hearing loss may be a first sign of impending deafness. A detailed eye examination may reveal uveitis in addition to conjunctivitis. In unclear cases of FCAS, placing the patient in a very cold environment for 15–20 minutes may induce an attack and rash within 30 minutes to several hours, with increased production of acute-phase reactants.
Formal diagnostic criteria for CAPS have not yet been defined. In order not to deny treatment and prevent potentially devastating damage to patients, genetic confirmation should not be a compulsory criterion. In Table 2 (above), we suggest criteria for potential clinical diagnosis. Large databases, such as the Eurofever registry, may be an aid in defining evidence-based criteria.12

