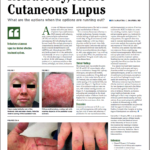
NEW YORK (Reuters Health)—Patients with cutaneous lupus erythematosus (CLE) should be monitored closely for other autoimmune conditions, researchers suggest.
Dr. Benjamin Chong, Dr. Linda Hynan and Elaine Kunzler of the University of Texas Southwestern Medical Center in Dallas analyzed data from 129 adults in the UTSW Cutaneous Lupus Registry (mean age, 49; 79% women). Individuals who met at least four American College of Rheumatology (ACR) diagnostic criteria for systemic lupus erythematosus (SLE) were excluded.
For the cross-sectional pilot study, autoimmune diagnoses were collected by patient history and a medical record review. During the six months following the initial study visit, participants were evaluated by specialists to confirm the diagnoses of concomitant autoimmune diseases.
As reported online May 2 in JAMA Dermatology, 23 participants (17.8%) were found to have coexisting autoimmune conditions. Thyroid disease (including Graves disease and Hashimoto thyroiditis) had the highest frequency at 4.7% (6 patients), followed by Sjogren syndrome (4 patients), rheumatoid arthritis (3), alopecia areata (3), and morphea (2).
One patient had rheumatoid arthritis, Sjogren syndrome and microscopic polyangiitis, and another had Sjogren syndrome and Guillain-Barre syndrome. Other conditions included immune thrombocytopenic purpura, microscopic polyangiitis, multiple sclerosis, pernicious anemia, and ulcerative colitis.
Coexisting autoimmune conditions were significantly more likely in patients with CLE who were white (odds ratio, 2.88), never smokers (OR, 3.28), had a family history of autoimmune disease (OR, 3.54), or a history of positive antinuclear antibody test result (OR, 4.87).
“We recommend that dermatologists treating patients with CLE maintain a low index of suspicion for presence of additional autoimmune conditions,” Kunzler (who will graduate from medical school this month) and Dr. Chong said in a joint email to Reuters Health.
“This can be done by inquiring about symptoms that are found in autoimmune conditions, especially those associated with autoimmune thyroid disease and inflammatory arthritis,” they explain. “Findings during clinical encounters that raise suspicion for autoimmune diseases should prompt dermatologists to have a low threshold to not only workup patients for coexisting autoimmune conditions, but also to communicate with and refer to appropriate specialists.”
“CLE is a complex disorder and care should be taken to minimize the disease burden and provide early identification of comorbidities,” they conclude.
Dr. Anca Askanase, Director, Columbia University Lupus Center in New York City, told Reuters Health that the study “further substantiates that CLE is part of the spectrum of autoantibody- mediated immune diseases.”
“It would indeed be interesting to know how many of the patients in this paper will ultimately develop SLE, since many of them meet several ACR criteria,” she said by email. “Additionally, (we don’t know whether) the Systemic Lupus International Collaborating Clinics criteria (were) evaluated for these patients.”
“As expected, a family history of autoimmune diseases and a positive anti-nuclear antibody test increased the likelihood of having an autoimmune disease,” she noted. “The association with white race and never smoker is somewhat unexpected.”
“The message of the paper is that a thorough review of systems and referral for appropriate testing is warranted,” Dr. Askanase said. “I would advocate that these patients should all see a rheumatologist.”
Reference
- Kunzler E, Hynan L, Chong B. Autoimmune Diseases in Patients With Cutaneous Lupus Erythematosus. JAMA Dermatology. 2018 May 2. https://jamanetwork.com/journals/jamadermatology/article-abstract/2679045?redirect=true