The AMA established the RUC process over the course of its normal activities as part of its research and data collection activities, for monitoring economic trends, and in connection and related to the CPT development process.
(click for larger image)
The Basics of the RUC Survey Process
When new codes are established or existing codes are revised by the CPT editorial panel, a survey of physicians providing that service is conducted by the relevant medical specialty society. The surveys are conducted under the auspices of the RUC. The ACR is an active participant in the process by conducting surveys for rheumatology services, analyzing the results and presenting recommendations to the RUC. Once the request is received to survey a code or code set, the ACR must follow a precise survey process that has specified timeframes as outlined by the RUC and AMA staff.
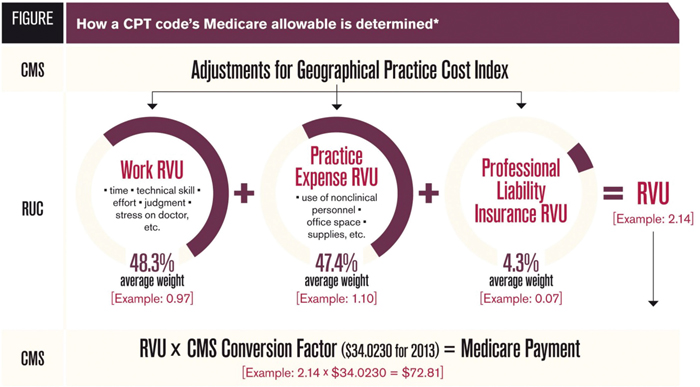
The purpose of the survey is to measure physician work involved in performing the procedure to determine an accurate relative value recommendation for the service. The AMA defines physician work as:
- Physician time it takes to perform a service;
- Physician mental effort and judgment;
- Physician technical skill and physical effort; and
- Physician psychological stress that occurs when an adverse outcome has serious consequences.
The key steps involved in the survey process include:
- Developing a description of the service and typical patient for each code being surveyed. These are called vignettes and are included on the questionnaire form distributed to survey participants.
- Society staff will have to identify a representative sample of physicians who are familiar with the service or procedure that is being evaluated. To be considered representative for the survey, samples must include a range of sub-specialization and generalists in the specialty (as appropriate for the codes being surveyed), practice circumstances and settings (e.g., solo practice, academic settings, large group practice) and relevant geographic areas.
- A set of reference codes that is representative of a broad range of services and work relative values will need to be selected that are well understood and commonly performed by members of the specialty. The work of the surveyed code will be compared to the work of the codes on the reference list.
- Surveys will need to achieve responses from at least 30 physicians. A high response rate lends heightened credence to the results and facilitates an easier process for the College to gain support for the code values.
- The survey results are reviewed and discussed with the RUC and CPT advisors, with final review from the ACR Committee on Rheumatologic Care to formulate specific recommendations for physician work value, procedure times and number/level of visits.
- The survey recommendation is submitted to the AMA for review by the panel.
- The ACR RUC advisor will present the recommendations at an RUC meeting (meetings are held three times per year).
- The RUC may take one of several actions: approve the specialty society recommendation, modify the recommendation or send it back to the specialty society or CPT advisors for further input/modification before submitting to CMS.
- The RUC’s recommendations for work values, practice expense inputs and PLI crosswalks are submitted to CMS in May of each year. The recommendations are confidential until CMS publishes them in the Final Rule in November.
- Code values go into effect in January of the following year.
The success and integrity of the RUC and CPT process is dependent on fairness and objectivity of the committee members. The ACR has advisors to both the AMA’s CPT Editorial Panel and the RUC who actively participate in the process to ensure development of CPT codes and appropriate value to procedures performed in rheumatology practices.