Diffuse alveolar hemorrhage (DAH), also rare but potentially fatal, can resemble ALP, but if hemoptysis is also present, consider DAH, Dr. Silver said. A falling hematocrit is a telltale sign of DAH, and rituximab has shown efficacy in its treatment.1
Risk factors for pulmonary arterial hypertension (PAH) in SLE include Raynaud’s phenomenon, anti-U1 RNP antibodies, anti-cardiolipin antibodies and anti-endothelial cell antibodies. High-risk patients can be screened with pulmonary function tests and echocardiogram, though the gold diagnostic standard is right heart catheterization.
A diagnosis occurs when a high pulmonary arterial pressure with a non-elevated pulmonary capillary wedge pressure and a pulmonary vascular resistance of greater than or equal to 3 Wood units are evident.
“You might have pulmonary hypertension on an echo or even on a right heart catheterization,” Dr. Silver said, “but if the [wedge pressure is elevated], it’s not PAH. It’s diastolic dysfunction or some other cardiac issue leading to pulmonary hypertension. Unless it’s PAH, you shouldn’t embark on PAH-specific therapy.”
More therapeutic options have emerged in recent years, he said.
“We now have a host of PAH-specific therapies,” Dr. Silver said. “Most people would either use monotherapy with an oral agent, or a dual combination oral therapy using both a PDE5 inhibitor and an endothelin receptor antagonist (ERA). This really requires the input of a PAH specialist. If patients are failing mono- or dual-combination therapy, that therapy needs to be escalated, and this usually requires a multidisciplinary approach.”
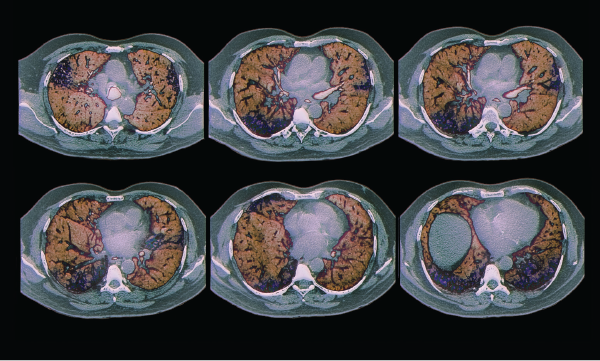
Colored computed tomography (CT) scans of axial sections through the chest of a 68-year-old patient with interstitial lung disease (diffuse parenchymal lung disease, DPLD). Parenchymal disease appears in less than 5% of lupus patients.
Zephyr / Science Source
Kidney Manifestations
Severe lupus manifestations in the kidney can prove challenging to manage, said Derek Fine, MD, a nephrologist and associate professor of medicine at Johns Hopkins, Baltimore. But he offered these suggestions on how to make the best of a challenging situation:

