First, the authors stress two overarching principles: 1) PtCs apply to patients who meet the EULAR definition for D2T RA (see Figure 1, left); and 2) the “presence or absence of inflammation should be established to guide pharmacological and non-pharmacological interventions.” Specifically, “concomitant fibromyalgia, osteoarthritis, and/or psychological conditions, nonadherence, and comorbidities like infections and cancer may contribute to the D2T state” and thus need to be considered when a patient isn’t responding the way we’d like.9
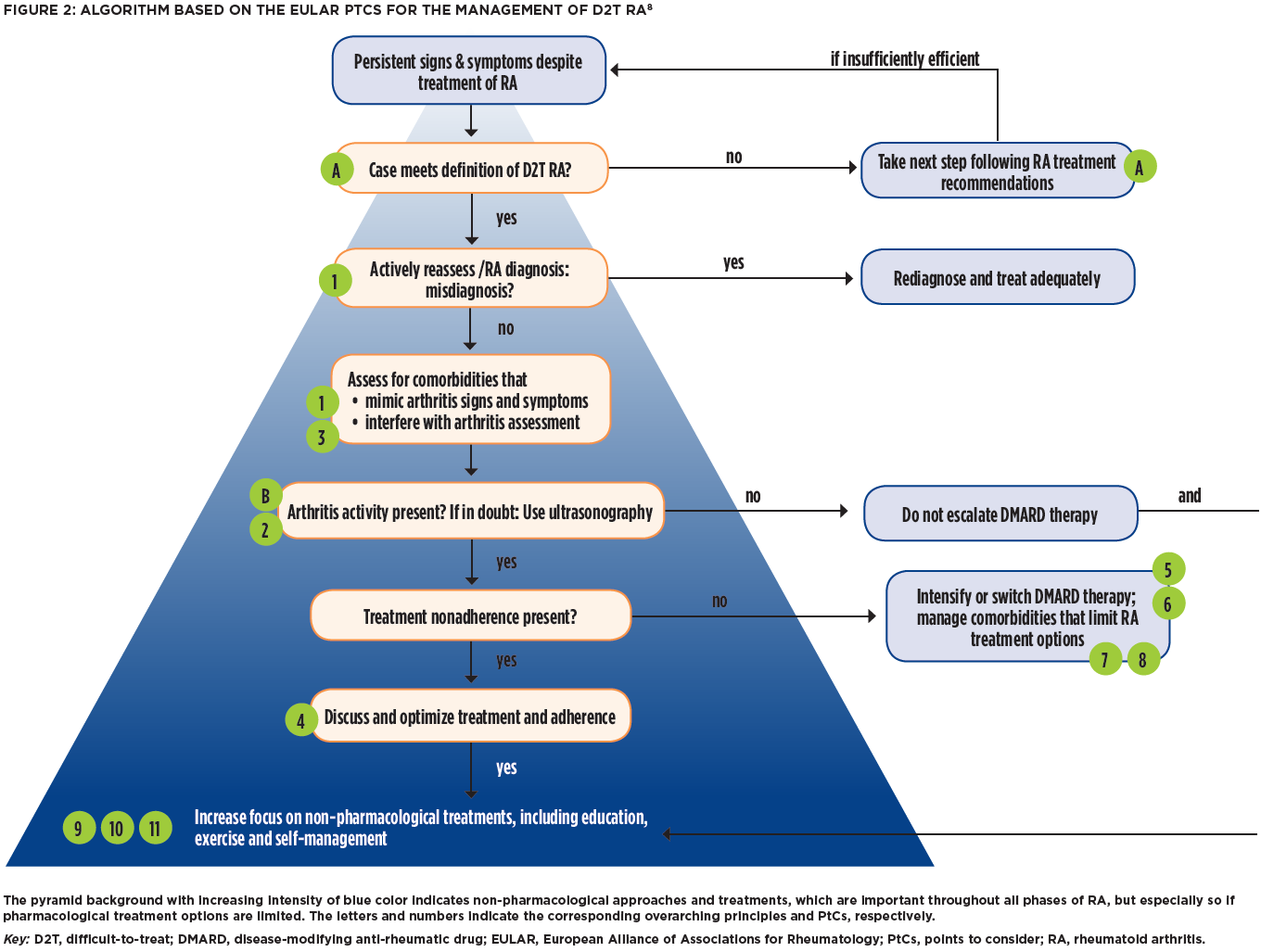
FIGURE 2. Click to enlarge.
When it comes to differentiating inflammatory from noninflammatory disease activity, ultrasonography can be a useful adjunct to physical exam, but the evidence for biomarkers and other imaging modalities is less convincing.10,11


