Postoperative Exercise (REHAB)
Immediately following THR and TKR surgery, muscle strength is typically less than preoperative levels and then begins to rebound by three months after surgery. Meier and colleagues reported isometric and isokinetic quadriceps strength deficits ranging from 15% to 41% compared with the uninvolved side three to six months post-op.7 Muscle strength deficits may remain as long as 13 years following TKR when compared to individuals’ uninvolved side and age-matched healthy peers. Persistent quadriceps (vastus lateralis) weakness has also been reported following THR.8
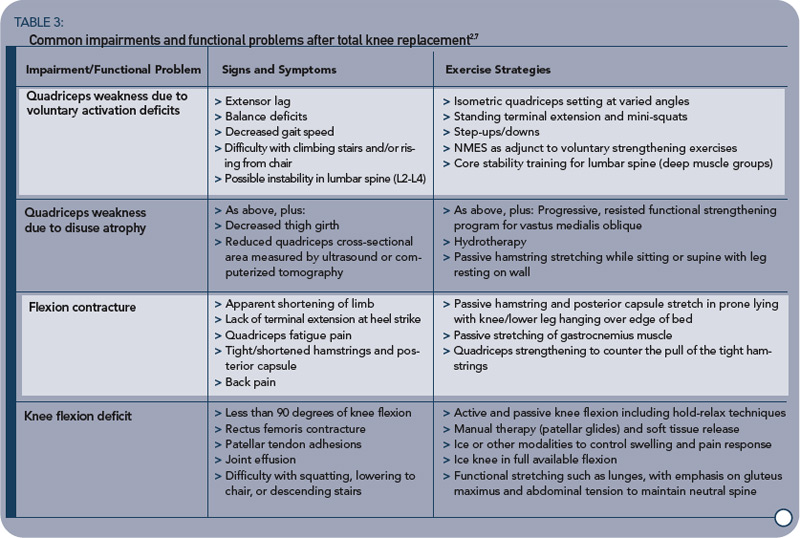
While quadriceps deficits, due to voluntary activation failure and muscle atrophy, are weakly linked to self-reported function, strong ties to functional performance (fall risk, stair climbing, and gait speed) have been identified.7 Similarly, deficits in hip abductor strength following THR are related to reduced functional performance, including postural control.9 A list of common post-THR/TKR impairments and functional problems and exercise strategies for overcoming them are in Tables 1 (p. 17) and 3 (above).


