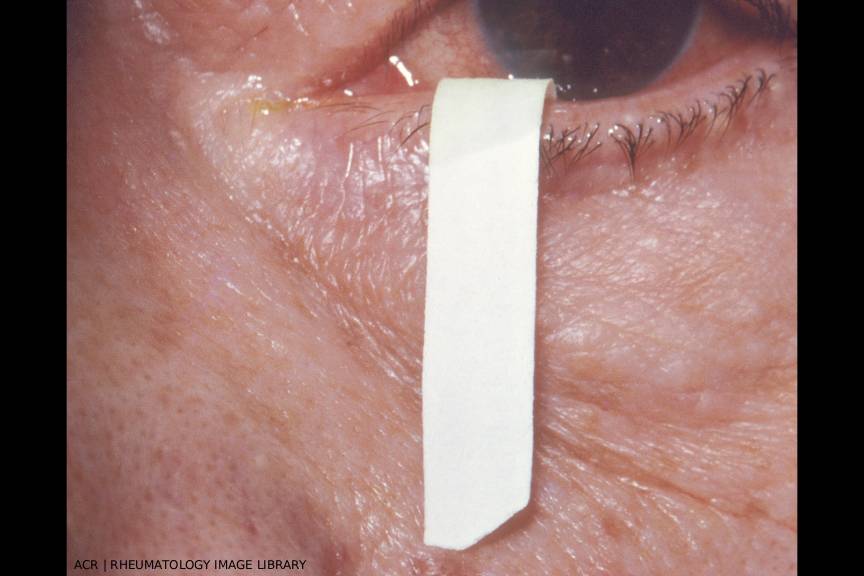
This image demonstrates the Schirmer test, which is used to detect deficient tear production of Sjögren’s disease. The filter paper strip is placed at the junction of the eyelid margins. After five minutes, 15 mm of paper should be moistened if tear production is normal, as shown here. If someone is older than 40, they may moisten between 10 mm and 15 mm. (Click to enlarge.)
Sjögren’s disease (SjD) is a systemic autoimmune disorder with clinical heterogeneity that challenges even the most experienced rheumatologists. SjD is an alternative name for Sjögren’s syndrome.1 The Sjögren’s Foundation, as well as many SjD experts, has advocated for this name change to underscore the fact that SjD is not just about dryness, but a distinct autoimmune disease with potentially serious outcomes. SjD includes both glandular and extra-glandular manifestations, such as interstitial lung disease (ILD), peripheral neuropathy and an increased risk of lymphoma. Despite the fact that it affects an estimated 0.1–0.6% of the population, SjD remains underdiagnosed and frequently mischaracterized, in part due to its insidious onset and overlapping symptomatology with other rheumatic diseases.
In this article, we explore practical approaches to the diagnosis and management of Sjögren’s disease with two experts at the Penn Sjögren’s Center, Perelman School of Medicine, University of Pennsylvania, Philadelphia: Chadwick R. Johr, MD, associate professor of medicine, and Dana DiRenzo, MD, MHS, assistant professor of medicine. Their perspectives provide a focused, practice-oriented lens for navigating the diagnosis and monitoring of SjD in the clinical setting.
TR: What symptoms really get your attention for a possible diagnosis of SjD?

Dr. DiRenzo
DD: I love to ask about salivary gland swelling and pain. When a patient responds with something like, ‘Oh yeah, I had to go to urgent care for a swollen parotid gland,’ or ‘swelling has been going on since my 20s,’ or ‘I had a salivary stone,’ or ‘the dentist said my glands are swollen’ … this clues me in to more of a glandular phenotype. It also gets my attention when a patient says they have been repeatedly diagnosed with mononucleosis or mumps without necessarily [being tested] for it.