TR: So would you recommend objective dryness testing in patients with an ANA of 1:160 and fibromyalgia symptoms but no dryness?
CJ: Yes, I absolutely would. If there is a reasonable chance that a patient could have SjD, I wouldn’t want to miss it. I would do a Schirmer’s test and sialometry in the office and then consider sending the patient to one of our cornea specialists for further testing. Using a slit lamp, fluorescence and lissamine green, they are able to report an ocular staining score (OSS), which is more sensitive for early dry eye changes than Schirmer testing.
TR: How do you diagnose seronegative SjD?
DD: Diagnosing seronegative SjD requires a minor salivary gland biopsy (lip biopsy).2
TR: How is seronegative SjD different than seropositive SjD?
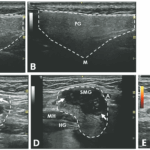
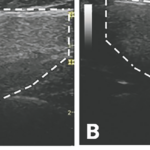
DD: Seropositive SjD is associated with more inflammation on labs. These are the patients with very high immunoglobulins, high inflammatory markers, hypocomp-lementemia and a positive rheumatoid factor. They have a lot of glandular swelling. They have high-grade inflammatory lesions on salivary gland ultrasound and an increased risk of lymphoma.
On the other hand, seronegative SjD patients tend to have normal labs and less organ involvement, but more neurologic findings like small fiber neuropathy and postural orthostatic tachycardia syndrome (POTS) symptoms.
I think in 10 years, we’re going to understand these entities much better with possibly even two different underlying mechanisms. It may be that they are two different pathophysiologic processes, and that’s what’s making the clinical trials hard. There are various mechanisms of action that could be coming into play. For example, dysautonomia could be part of the pathogenesis that is part of the dryness seen in patients without positive serologies.
CJ: In my mind, seropositivity is associated with more badness—significant organ manifestations, like ILD [interstitial lung disease], kidney disease and lymphoma. But seronegative patients can still develop any of these things. In this regard, you can think of it like rheumatoid arthritis (RA). Seropositive RA patients have a greater risk of developing extra-articular manifestations, but the seronegative patients can get these too.
TR: As you know, not all patients referred to us for dryness have SjD. What else is on your differential in these cases?
DD: Medications are the most common cause of dryness overall. Common culprits include tricyclic anti-depressants, overactive bladder medications, diuretics, antihistamines … the list goes on. There’s a great UpToDate article on this.