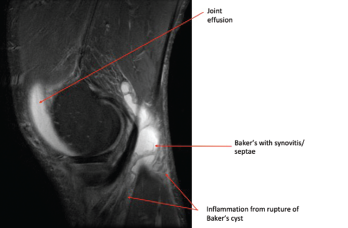
Photo 2: This MRI of the right knee shows a large joint effusion and a ruptured Baker’s cyst with synovitis.
In patients with Lyme arthritis today, synovitis is usually the presenting manifestation of Lyme disease, and a history of suspicious tick bite or classic erythema migrans skin lesion is often lacking. Patients with Lyme arthritis rarely have a history of prior treatment for Lyme disease, because early treatment largely prevents the progression of infection to clinical arthritis. Unlike patients with early Lyme disease, who typically present in the late spring and summer, Lyme arthritis patients may present at any time of the year.
Patients of any age may develop Lyme arthritis, but children are particularly affected, with 35% of cases occurring in 10- to 14-year-olds, and older adults are also increasingly affected.1 Children may have more acute presentations. Adult Lyme arthritis patients generally don’t have the severity of pain that occurs in patients with septic arthritis caused by such bacterial organisms as Staphylococcus aureus.