Burkholderia pseudomallei bacteria on a color-enhanced scanning electron micrograph (SEM). Image Credit: Eye of Science / Science Source
Burkholderia pseudomallei, the causative agent of melioidosis, is endemic in Southeast Asia and northern Australia.1 In recent years, the incidence of melioidosis has increased worldwide. Septic arthritis is a rare, but well-recognized, manifestation of melioidosis.
Case Report
A 49-year-old woman with known diabetes was admitted elsewhere with uncontrolled diabetes and fever. She was found to be in diabetic ketoacidosis. During her hospital stay, she had acute onset of severe pain, swelling and redness over the right shoulder joint. The shoulder joint was surgically drained, empiric parenteral antibiotics were initiated, and the patient was transferred to our hospital for further management.
On examination, she was febrile, the right shoulder was tender and warm, and all range of movement was severely restricted. There was also erythematous swelling of the right second proximal interphalangeal (PIP) joint, and diffuse swelling and tenderness over the left calf area.
(click for larger image)
Laboratory results included the following: hemoglobin, 9.8 gm/dL; leukocyte count, 13,400 cu/mm3 (90% neutrophils); platelet count, 4.36 cu/mm3; ESR, 106 mm/hr; CRP, 96 mg/dL; SGPT, 48 IU/L; creatinine, 0.8 mg/dL; rheumatoid factor and anti-CCP antibody were both negative. Lower limb color Doppler ultrasonography showed a lower left limb intramuscular fluid collection suggestive of an abscess.
An MRI of the right shoulder showed multiple abscesses with osteomyelitic changes (see Figures 1 and 2).
The synovial fluid culture from the shoulder, from the referring hospital, showed gram-negative bacilli on smear, but the organism was not identified. She was switched to injectable cefipime and tazobactam.
She underwent incision and drainage of the right shoulder joint and the left leg abscess. On the third postoperative day, she developed acute-onset tachypnea, and a chest X-ray showed changes of acute respiratory distress syndrome (see Figures 3, 4 and 5). The patient was intubated and treated with parenteral meropenem. However, she became anuric and succumbed to hyperkalemia-induced arrhythmia and cardiac arrest.
The day after her death, bacterial culture reports confirmed the growth of Burkholderia pseudomallei (B. pseudomallei) from the synovial fluid.
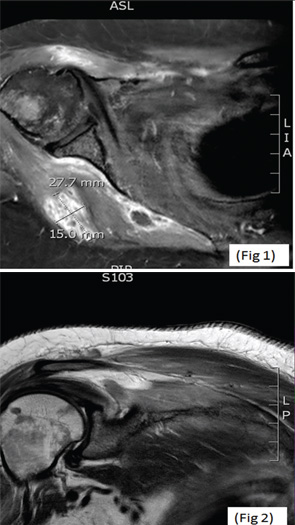
(click for larger image) MRIs of the right shoulder showing a collection within the right axilla (Fig. 1, top) and hyperintense signals from the head of the right humerus (Fig. 2).
Discussion
Melioidosis, also known as pseudoglanders or Whitmore’s disease, is caused by a gram-negative bacillus previously classified under genus pseudomonas—B. pseudomallei. It was identified in Burma in 1911 by Whitmore and Krishnaswami. It is classically characterized by the development of pneumonia and multiple abscesses, with a mortality rate as high as 40%. Melioidosis is an important cause of community-acquired sepsis in Southeast Asia and Australia and is classified as a Group B bioterrorism agent.1,2