Similar Treatments for Many CSS Entities
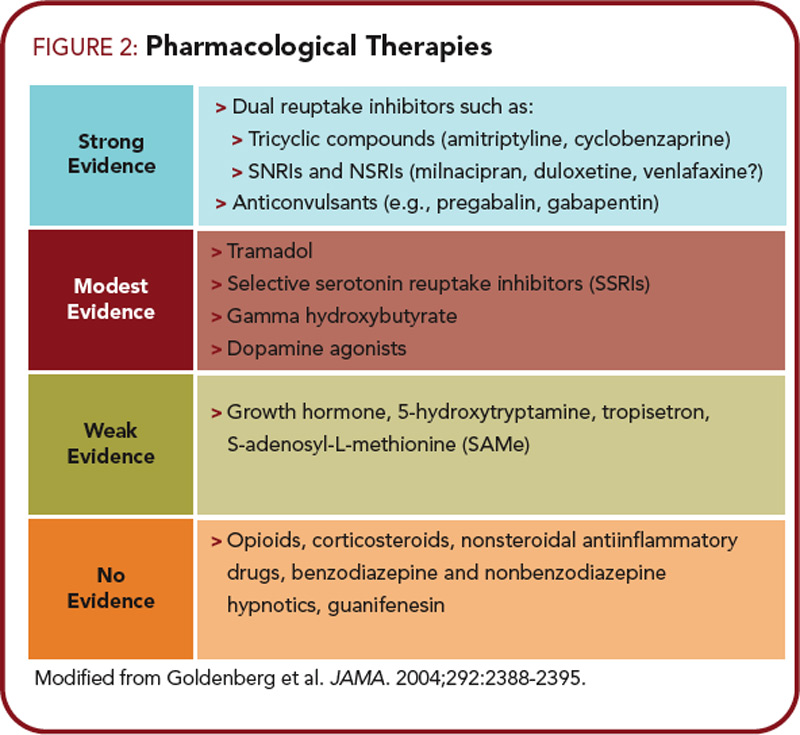
Several drug and nondrug therapies have been shown to be effective for most of the CSS disorders, further reinforcing that this may be a large overlapping disorder rather than several separate ones. Among classes of drugs, substantial data suggest that tricyclic compounds are effective for treating most of the conditions noted.37-39 Newer serotonin–norep – inephrine reuptake inhibitors such as duloxetine and tramadol have similarly been shown to be effective across a broad range of these conditions.40 Interestingly, duloxetine had much earlier been shown to be helpful in treating the pain associated with depression, which is not surprising. The alpha-2- delta ligands, such as pregabalin and gabapentin, are also being shown to be efficacious in a wide range of these entities.41