Editor’s Note: This article initiates a new department in The Rheumatologist that will focus on regional musculoskeletal disorders that may be seen by both rheumatologists and orthopedic surgeons. To promote the care of these patients and facilitate communication between rheumatologists and orthopedists, these articles will provide focused discussions of clinical and radiographic findings and describe management principles from the orthopedic perspective. We hope that this series will increase awareness of the diversity and complexity of painful musculoskeletal conditions and enhance patient outcomes through improved collaboration between medical and surgical specialists.


Meniscus Extrusion
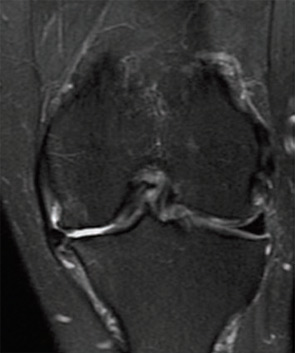
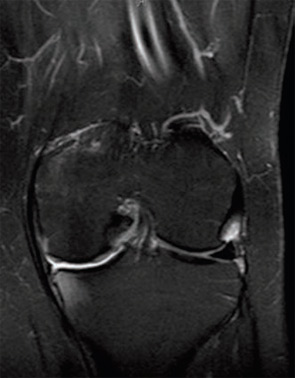
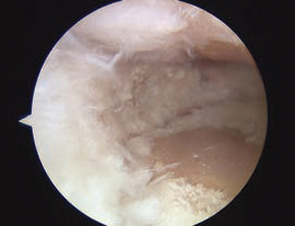
Meniscus extrusion is a common, but often overlooked, source of joint line pain that can be associated with knee arthritis. An extrusion occurs when the meniscus subluxates out of the tibiofemoral joint into the adjacent gutter. A meniscus is at risk for extrusion when there is arthritis in its compartment and when pathology of the meniscus, particularly a tear, can weaken its structure.
