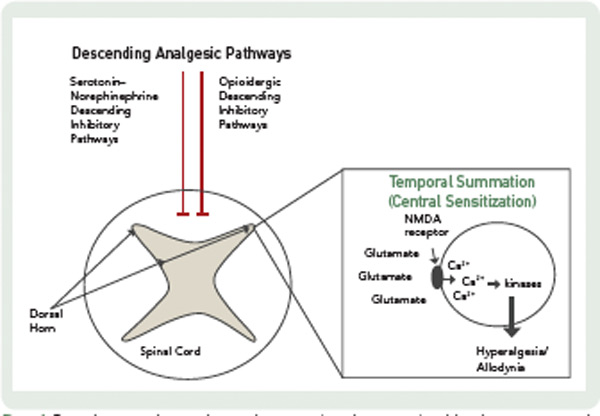
In addition to a loss of descending analgesia, some fibromyalgia patients also exhibit enhanced temporal summation, otherwise known as central sensitization. Temporal summation describes the phenomenon by which repetitive painful stimuli lead to the lowering of pain thresholds and heightened pain sensitivity. This process is mediated by the excitatory neurotransmitters, glutamate and substance P. These molecules activate N-methyl-D-aspartate (NMDA) receptor channels, leading to an influx of calcium ions which activate kinases that lower the pain threshold. These changes in CNS processing have implications for pharmacological and nonpharmacological treatment.
Pain Mechanisms in RA
In contrast to the situation in fibromyalgia, the role of augmented CNS pain processing in systemic inflammatory diseases, such as RA, is not well established. Several studies have reported that the prevalence of fibromyalgia is higher among patients with rheumatic diseases associated with peripheral pain and inflammation than among control populations. The prevalence of fibromyalgia ranges from 13% to 22% among patients with RA, compared to only 2.5% for healthy controls.6,7 Which RA patients are at risk for secondary fibromyalgia is not clear, although a recent study suggested that the development of fibromyalgia in RA is associated with psychosocial distress, comorbidities, and sociodemographic disadvantages.8