
Other Clinical Features
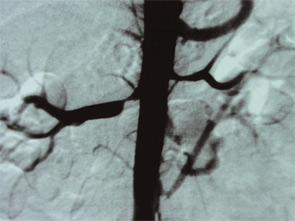
Gastroenterology: As well as Budd-Chiari syndrome—of which APS is a major cause—more focal hepatic thrombosis is frequent, and abnormal liver function tests are frequent in poorly controlled APS. Idiopathic cirrhosis has also been reported in some patients. Celiac axis arterial stenotic lesions were first fully appreciated in angiographic studies of renal artery stenosis. The classical symptoms of post-prandial mesenteric angina were present in most—though not all—of the patients.
Skin: Livedo reticularis is not only an important marker for APS; it could well be a risk factor in itself. Patients with sero-negative APS—as described below—include some with florid livedo. Thrombosis—particularly DVT and skin vessel thrombosis—leads to skin ulceration. For those who conduct skin ulcer clinics, it is clear that a subset of patients exists in whom chronic skin ulceration could well be improved with anticoagulation.

