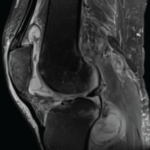
The researchers said that a chest radiograph “is not sufficiently sensitive for detecting bronchiectasis or other lung abnormalities associated with NTM disease.” They recommended that clinicians obtain a noncontrast chest computed tomography (CT) scan before giving this therapy to patients who may be at risk.
Dr. Iseman said that physicians should consider any patient with a history of chronic cough or recurrent pneumonia as being at potential risk for NTM with initiation of anti–TNF-α therapy. Patients at risk should be screened by chest X-ray and CT scan, with additional sputum screening for AFB. Any patient needing treatment with anti–TNF-α should be referred to an infectious disease specialist or pulmonologist before initiation of the therapy, Dr. Iseman said.
Dr. Winthrop and colleagues also reported the results of a survey of infectious disease physicians, which found that the cases of NTM disease associated with anti–TNF-α therapy “occur twice as frequently as cases of TB,” and that these diseases are likely not reported as frequently to the FDA as reports about TB.1
While advising that it is unclear from their research whether it is safe to reinstitute anti–TNF-α therapy in patients diagnosed with NTM, Dr. Winthrop and colleagues note that “it is not possible to definitively conclude that [the therapy] causes or is associated with NTM disease.” Certainly, they said, NTM is underreported, and their findings “highlight that these cases are occurring in such patients, often with devastating outcomes.”1
Latent TB
Although the incidence of TB in the United States is declining within the general population, certain populations are at high risk: immigrants, minorities, the homeless, substance abusers, the elderly, healthcare workers, and those who are immunocompromised due to AIDS, oncology therapy, organ transplantation, or use of biologics, Dr. Iseman said.
TB is spread human to human and is an airborne infection, he said. “Depending on the reception that your immune system gives to the infection, it may progress rapidly in multiple weeks to a near life-threatening disease. For patients infected with AIDS who are then infected with TB, death can occur within four weeks.” For others, TB can be dormant for any length of time, even up to seven decades. “The obligation to screen for latent TB before putting someone on biologics is explicit,” he said.
The tuberculin skin test (PPD) is often used for screening of latent TB, but it is neither sensitive nor specific. The skin test cross-reacts with people who have had BCG vaccination, given in most parts of the world but not in the United States. About 25% of people with active TB do not react positively to the tuberculin skin test, he said.