An anemia workup was suggestive of anemia of chronic disease. Further testing included serum electrophoresis that did not reveal any monoclonal spike. Interestingly, the subtypes of IgG found a mildly decreased serum IgG1 (333 mg/dL; normal range 382–929 mg/dL). Both C3 and C4 serum complements were significantly reduced (C3 57 mg/dL; normal range 83–193 mg/dL; C4 -4 mg/dL; normal range 15–57 mg/dL).
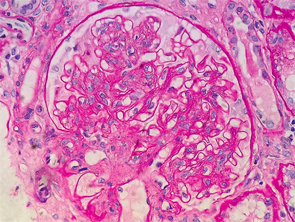
Figure 1: Renal biopsy. H&E staining: enlarged glomeruli, mesangial expansion with diffuse increased cellularity; glomerular basement membranes irregularly thickened, but no vasculitis, necrotizing lesions, crescents or hyaline thrombi were seen within the capillary loops.
Creatinine worsening accompanied by nephrotic range proteinuria, low serum complements levels, positive ANA, SSA/SSB and anti-histone antibodies in the context of active RA disease suggested an autoimmune process as a plausible cause of current renal failure.

